 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Quality of life and self-perceived oral health among workers from a furniture industry Cristina Gomes de Macedo1, Dagmar de Paula Queluz2
1DDS, Master student, Piracicaba Dental School, University of Campinas (UNICAMP), Brazil 2DDS, MSPH, PhD, Professor, Department of Community Dentistry, Piracicaba Dental School, University of Campinas (UNICAMP), Brazil Received: March 09, 2011 Code Number: os11046 Abstract
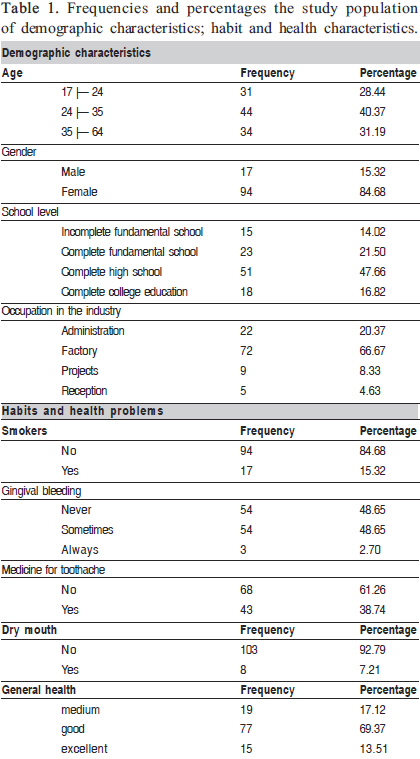
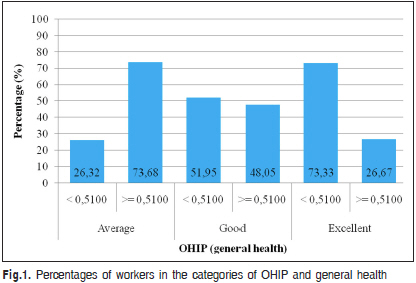
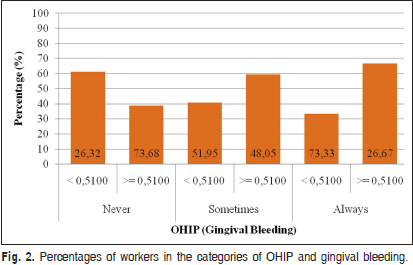
Oral health problems have more and more been recognized as important causers of negative impact to workers in the daily activities and quality of life. Keywords: oral health, quality of life, self assessment (Psychology), occupational health. Introduction Oral health problems have more and more been recognized as important causers of negative impact to workers in their daily activities and quality of life1-2. The orofacial region is usually an area of significant concern because it draws the most attention from other people in interpersonal interactions and is the primary source of vocal, physical, and emotional communication3 . The Oral Health Organization has recognized that oral diseases cause pain, psychological suffering, social constraints and privations, leading to damage in an individual and collective level4 . Few studies have so far investigated the relationship between the oral conditions and their impact on people’s life, but in recent years, the use of clinical indicators (e.g: gingival bleeding, caries, tooth loss) in epidemiological studies has been widely recommended. However, these clinical indicators have been frequently used only to determine the presence or absence of the disease/ condition, but their impact on patients and populations have not been investigated5. Measuring the impacts of oral conditions on quality of life is an important part of oral health needs assessment. There are some instruments described in literature for measuring the impact of oral health on the quality of life. However, these instruments differ with respect to size, content, structure of the response form scale and methods for obtaining the scores. A common problem in assessing the strength of the measures obtained with these instruments is that researchers usually do not specify why it is important to evaluate a specific clinical indicator in the studied population and they often only reproduce existing methodologies and compare their data with those of previous studies6 . Validated and reliable instruments for measuring subjective oral diseases were introduced in the 1990s to supplement the clinical indicators used routinely. They are used for collecting oral health data at both individual and population levels, and can be applied in education, preventive and curative programs as well as by other health care professionals7. Subjective indicators can be either onedimensional, when they cover only one aspect (e.g.: chewing difficulty or pain intensity) or multidimensional, when they encompass different dimensions (e.g.: pain, constraints and psychological well-being of individuals). One of the most widely used indicators in different cultures and sociodemographic profile is the oral health impact profile (OHIP). Developed by Slade and Spencer8 , the proposed questionnaire measures dysfunction, discomfort and disability attributed to oral condition. Originally composed of 49 items, the conceptual index involves seven dimensions: functional limitation (e.g., chewing difficulty), physical pain (e.g., toothache), psychological discomfort (e.g., self-confidence), physical disability (e.g., food restriction), psychological incapacity (e.g., affected concentration), social disability (e.g., is less lenient with others) and functional incapacity (e.g., become completely incapable functionally). The questionnaire is answered on a five-point Lickerttype, scale (always, often, sometimes, rarely and never). A short OHIP version has emerged as a powerful instrument in the subjective assessment of oral health related to the quality of life. Containing 14 items, this version is preferred over OHIP-49 by many researchers because of its convenience and validation. The short version of this instrument, the OHIP14, was developed by Slade in 19979, and validated for use in adult population in England10 and Scotland11. It was translated and trans-culturally adapted in 10 languages12-17 including Portuguese14. Studies9,18 have shown that OHIP-14 presents good psychometric properties when employed in more distinct populations. Interest in the oral health of workers has increased due to need of knowing the oral health profile of this population group as little information is available about this subject. There is still the need to understand how employees perceive the influence of oral health on their quality of life. This information is relevant for the development of oral health strategies that meet the specific needs of this population, benefiting their well-being and general health. Thus, the aim of this study was to identify the profile and self-perceived oral health among workers from a furniture industry. Material and methods The research protocol was reviewed and approved by the Ethics Committee of the University of Campinas, under the protocol number 009/2009. All 170 workers from a furniture industry located in the municipality of Itatiba, SP, Brazil, were invited to participate in the study. The investigation was designed as a crosssectional study and the data collection was held through questionnaires focusing questions on profile and selfperceived oral health. The demographic characteristics comprised questions about age, gender, school level (incomplete fundamental school, complete fundamental school, complete high school, complete college education), occupation (administration, production, project, reception). Habits and health problems comprised questions about smoking (no, yes), gingival bleeding (never, sometimes, always), use of medications for toothache relief (no, yes), dry mouth (no, yes), general health (medium, good, excellent), mean frequency of toothbrushing (one, two, three, four, more than four times/day, never). Self-perceived oral health was evaluated using OHIP 14 short form9. The OHIP is composed of 14 items divided into 7 conceptual dimensions: functional limitation (items 1 and 2), physical pain (items 3 and 4), psychological discomfort (items 5 and 6), physical disability (items 7 and 8), psychological disability (items 9 and 10), social disability (items 11 and 12) and physical limitation (items 13 and 14). The answers of the workers to the OHIP questionnaire were analyzed using a Lickert-type scale in which answers are encoded into five categories. Each category received a score between 0 and 4, which was multiplied by the weight of each question: 0 = never 1 = almost never, 2 = sometimes 3 = with reasonable frequency and 4 = very frequent9 . The application of the questionnaire was accompanied by a psychologist of the Department staff in different shifts, after instructing the workers on how to fill out the questionnaire. During conduction of the study, the identities of workers were shielded in the questionnaires. All procedures were carried out with treatment ensuring reliability and credibility to the worker. Descriptive statistics (frequency distribution, average, standard deviation) were used to characterize the workers. Epidemiological studies using the OHIP have found that oral diseases are associated with increasing levels of impact on well being. Based on the answers to the OHIP, the workers were divided into two major groups: no impact (0 = never, 1 = almost never and 2 = sometimes) and impact (3 = with reasonable frequency and 4 = very frequent). If at least one dimension was scored 3 or 4 the worker was considering as belonging to the impact group. Data were tabulated using Excel19 software (2007) and were then analyzed using the SAS20 (2002) system. The Mantel and Haenszel Chi square tests, Fisher’s exact test, and the coefficient V Cramer were used to analyze the association between OHIP and demographic characteristics (age, gender and school level) and the related variables measures health. A significance level of 0.05 was adopted for all tests. Results From the 170 individuals working at the furniture industry, 111 accepted to take part in the study. The industry presents a variation of 10-15 workers per year and many outsourced workers in other distant occupations of the search local. The age range was from 17 to 64 (mean age 31.38±9.34 years). The majority of workers (68.81%, n = 75) were under the age of 35 years and 31.19% (n=34) were over this age (Table 1). The majority of workers were male (n= 94, 84.68%). With regard to school level most workers (64.48%, n = 69) had at least graduated from high school and 23 workers (21.50%) had completed the fundamental school (Table 1). Regarding the occupation in the industry, most were production workers (n=72, 66.67%) covering sectors like polishing, maintenance, glass factory, carpentry, sorting, warehouse and management (Table 1). The majority of the workers (n=94; 84.68%) were nonsmokers. The mean frequency of tooth brushing (number of times per day) was 3.19 (Table 1). Fifty-four workers (48.65%) had never had gingival bleeding and only 3 workers (2.70 %) said to have gingival bleeding frequently. The most serious instances with frequencies are only three cases being that, among those who had bleeding, the majority (n = 54) said to be a low frequency event (Table 1).About medications for toothache relief, 68 workers (61.26%) had never used while 43 workers (38.74%) had already used some kind of medications for toothache (Table 1). There was no significant association between the use of medications for toothache relief and gingival bleeding (p=0.729) or dry mouth (p=0.704); but it was positively associated with smoking (p=0.007). In relation to dry mouth, the frequency of workers with dry mouth was low (n=8, 7.21%) against a total of 103 workers (92.79%) who had never experienced this condition (Table 1). About the general health, 15 workers (13.51%) considered their general health as excellent, 77 workers (69.37%) considered as good and 19 workers (17.12%) considered as medium (Table 1). As much as 92 workers (82.88%) of the workers considered their general health as excellent or good. However, regarding the impact of oral health on quality of life, the mean OHIP value of this group was 1.74, which is much higher than the mean value of 0.51 recorded for the total population (Figure 1 and Figure 2). The Fisher’s exact test did not find significant association between the demographic characteristics and the OHIP value; such a difference was only detected using Chi square Mantel and Haenszel test, which are more specific to test the hypothesis of absence of linear association between the measures assessed. There was significant linear (p<0.01) association between OHIP values and self-assessed general health. This association can be illustrated by the fact that people who perceived their general health as medium (73.68%) recorded OHIP values above the mean value for the total population while those who perceived their general health as good or excellent (26.32%) recorded OHIP value below the mean value for the total population (Figure 1). Significant association was found between the OHIP value and gingival bleeding (Figure 2), as higher incidence of gingival bleeding coincided with higher OHIP value. We could observe the same inversion that we observed in the association of OHIP and general health. Lower OHIP values were most often associated with workers who had never had gingival bleeding (73.68%), while higher OHIP values were most frequently associated with workers who always have gingival bleeding (73.33%) (Figure 2). Discussion The analysis of the demographic characteristics of the studied population revealed that the majority of the workers were young (<35 years), male and had at least graduated from high school. The Brazilian Formal Worker Profile prepared by the Ministry of Labor and Employment’s Social Service for Industry traced the full picture of the reality of Brazilian formal workers in 5,500 municipalities21. In 2003, the evolution of employment by gender did not present major differences. However, despite the participation of women in the workforce in recent years, the number of formal male employees remains largely superior to female workers. In 2003, for example, the number of formal work spots occupied by men was 50.3% higher than those occupied by women. Regarding the behavior of formal workers according to the level of education, employment opportunity is lower in the lower levels of education21. This dynamics can be explained by two factors: firstly, we could be facing a supply of qualified workers. The second factor is that workers with the highest level of qualification would be required due to technological modernization21 . There was a prevalence of non-smokers in the studied population. Prevalence of tobacco use has declined in some high-income countries, but it continues to increase in low-income and middle-income countries, especially among young people and women. Undoubtedly, the increasing number of smokers and smokeless tobacco users among young people in some parts of the world will considerably affect the general and oral health of future generations. The prevalence of tobacco use in most countries is higher among people of low educational background and among poor and marginalized people22 . The mean frequency of toothbrushing (3.19 times per day) found in this study is considered as an indicator of good oral hygiene habits and concern about health and appearance. Hugoson et al. 23 in 2005 compared data on dental care habits and knowledge of oral health in four cross-sectional epidemiological studies carried out in 1973, 1983, 1993, and 2003. A questionnaire about dental care habits and knowledge of oral health was used in connection with a clinical and radiographic examination. The same questions were used in all four studies. The knowledge of the etiology of dental diseases did not change much between 1973 and 2003. The frequency of tooth brushing increased from 1973 and in 2003 more than 90% of all investigated individuals brushed their teeth twice or once a day. The use of dental floss and toothpicks decreased in 2003 compared with 1983 and 1993. In 2003, almost all individuals used fluoride toothpaste. It was obvious that the dental team constituted the main source of oral health information. For the 20-30year-old age group, information from friends and relatives was also important. In the 3-20-year-old age group, up to 45% of the individuals consumed soft drinks every day or several times a week. We did not find evidence of association between demographic variables with the workers’ self-perceived general health, i.e. the different strata of age, gender and school level did not have an important influence on the general health. As the workers did not present so distinct demographic characteristics, as expected, these characteristics did not exert an effect on the concept of general health. Contributed considerably to the absence of effect, the uniformity of the population, which was predominantly composed of men aged between 17 and 64 years, with a predominantly high school level for the Brazilian standards, since more than 85% of the workers had completed fundamental education and 64.48% had at least graduated from high school. Good health is a major resource for social, economic and personal development. Political, economic, social, cultural, environmental, behavioral and biological factors can enhance or impair health. Almost forty percent of employees had already used medications for toothache relief, which is not negligible a percentage, and 57 workers said to always or sometimes suffer from gingival bleeding. There are few reports in the literature about oral health conditions in adults as well as a shortage of structured collective health programs for this economically active population. However, there is a consensus that adults constitute the vast majority of the population that demand for dental care and influence the behavior of their dependants24 . Oral health-related quality of life can be assessed positively, by measuring satisfaction with mouth, or negatively, by measuring oral impact on the performance of daily activities. Slade et al.25 compared subjective oral health of adults in the UK and Australian populations. Cross-sectional studies were conducted with people aged 18+ years in the 1998 UK Adult Dental Health Survey and the 1999 Australian National Dental Telephone Interview Survey. Subjective oral health was measured using the 14-item Oral Health Impact Profile questionnaire (OHIP-14). While the percentage of adults reporting adverse impacts of oral health was similar, Australians reported a larger number of impacts and more severe impacts than dentate people in the UK. Differences in the number and severity of impacts between the two populations may be an artifact of different data collection methods or may reflect relatively subtle socio-cultural differences in subjective oral health between these populations. Although the effect of disorders on psychological wellbeing is well-known, there are few studies focusing on oral conditions at the worksite. Another study examined the association between psychological well-being and oral conditions of Japanese workers. A cross-sectional study was performed using data from 1,381 Japanese civil service officers aged 20 to 59 year. Results did not show that psychological well-being was associated with oral conditions measured by clinical indicators. However, an association was found between some oral symptoms and psychological wellbeing. Absence of oral symptoms seems to be related to better psychological well-being26 . Using a questionnaire containing a spontaneous smiling photograph of the participant, Geld et al.27 investigated selfperception of smile attractiveness to determine the role of smile line and other aspects correlated with smile attractiveness and their influence on personality traits, concluding on the psychosocial importance and the dental significance of an attractive smile. Brennan et al.28, in a study with middle-aged and older adults, investigated tooth loss and chewing ability and their association with oral- and general-health-related quality of life and life satisfaction. The authors concluded that chewing ability was related to oral-health-related quality of life and general health, possibly reflecting the impact of chewing on food choice and enjoyment of meals and diet, and also indicating the importance of oral health to general well-being. Oral health deficits can have a significant effect on workers’ general health and their ability to carry out normal activities. Significant differences were found between the mean OHIP value and general health in this study. Lower OHIP values were most often associated with excellent selfperceived health and higher OHIP values were most frequently associated with medium self-perceived health. This difference between the average and median is quite representative in light of the magnitude of value and possibly be unduly influenced in the case of average by highest values. The standard deviation of 2.69 indicates that the variability is bigger than the average, which characterizes a high variability in data, although a large proportion of people recorded a very low OHIP value. General health indicator was incurred and in conjunction with OHIP want to allowed assessment on the quality of life. In another study, Quandt et al.29 observed that although farm workers have been found to lack access to dental care, few studies have documented their oral health status or its impact on quality of life. This research describes the oral health problems experienced and oral health care received by Latino farm workers in North Carolina, and explores the association between oral health and quality of life. Data were collected using face-to-face interviews from a representative sample of 151 farm workers; data included oral health-related quality of life (OHIP-14) and general health-related quality of life (SF-12 Health Survey). Workers reported a high number of unmet needs: 52% reported caries, and 33% reported missing teeth. These findings indicate that the high rate of unmet oral health needs is associated with poorer farm worker quality of life. The consequences of suffering on-going dental pain for work performance, sleep, and nutritional status are unknown. Kieffer and Hoogstraten30 studied the association among oral health, general health, and quality of life. The Oral Health Impact Profile (OHIP-49) and the RAND-36 were distributed amongst 118 psychology freshmen. Additionally, two single items self-rated general health (SRGH) and self-rated oral health (SROH) - were administered. Kruskal-Wallis and Mann-Whitney U-tests were used to evaluate differences between SRGH and SROH categories, regarding OHIP subscale scores and RAND subscale scores. More than 75% of the subjects rated their oral and general health as good. Mean OHIP scores and RAND scores indicated a relatively good oral- and general health-related quality of life, respectively. The correlation between oral and general health was weak. The findings suggest that oral health, general health, and quality of life have different determinants. Furthermore, oral health and general health appear to be mostly unrelated in this seemingly healthy population. It is proposed that if no apparent disease is present, oral and general health must be regarded as separate constructs. The use of subjective indicators in dentistry has been increasing. A population-based cross-sectional study in the city of Chapecó, Santa Catarina State, Brazil, analyzed the relationship between oral health conditions and quality of life in 35-44-year-old adults (n = 622). Oral health status was found to interfere in the daily routine of 20.7% of participants and was more severe for 11.4%. Household crowding, low-income neighborhoods, female gender, and orofacial pain in the previous six months were associated with higher interference in quality of life. The use of subjective indicators in public health services helps planning the delivery of oral care to priority groups31 . Significant differences were found between the mean OHIP value and gingival bleeding in this study. Higher OHIP values were most often associated with workers who always had gingival bleeding. Several studies have linked periodontitis and consequently the gingival bleeding with numerous diseases, such as: premature birth and low weight of newborn children, lung disease, osteoporosis, stroke and diabetes. Thus, gingival bleeding affects the workers’ selfesteem and consequently their quality of life, interfering in their social and labor coexistence32-33 . Drumond et al.32 evaluated the potential impact of periodontal disease on quality of life in diabetics. A total of 159 dentate diabetic individuals registered at the Municipal Hospital in Itaúna, MG, Brazil, were examined and interviewed. The clinical periodontal parameters recorded were: gingival bleeding, probing depth, and clinical attachment level. The OHIP-14 form was used to evaluate the impact of periodontal disease on quality of life. Association between diagnosis of periodontal disease and impact on quality of life was significant in individuals with periodontitis (p < 0.001). Gingival bleeding, probing depth, and clinical attachment level > 4mm were associated with intensely negative impact on quality of life (p = 0.013, p < 0.001, and p = 0.012 respectively). Diabetics with mild-to-moderate and advanced periodontitis had more negative impact on quality of life than those who were periodontally healthy or with gingivitis. Another study33 assessed the periodontal health status in the Danish adult population, analyzed how the level of periodontal health is associated with age, gender, urbanization, socioeconomic factors, and dental visiting habits, and compared the periodontal health status of Danish adults with that of adults in other industrialized countries. Using a cross-sectional model, a random sample of 1,115 Danish adults aged 35-44 years and 65-74 years. Data were collected by means of personal interviews and by clinical examinations in accordance with the World Health Organization Basic Methods Criteria. The clinical examination revealed a low prevalence of healthy periodontal conditions in both age groups: at age 35-44 years 7.7% and at age 65-74 years 2.4% had healthy periodontal conditions. A high proportion of the elderly had scores of severe periodontal health; more than 82% of older participants had pockets of 4-5 mm or deeper against 42% in younger adults. In both age groups, the mean number of teeth with periodontal pockets deeper than 4-5 mm was high in individuals with low education. The multivariate analysis showed that participants with low or medium levels of education had significantly more teeth with shallow and deep pockets than those with high education. People with regular dental visiting habits had fewer teeth with gingival bleeding, shallow and deep pockets than individuals with irregular dental visiting habits. The authors concluded that reorientation of the Danish dental health-care services is needed with further emphasis on preventive care, and public health programs should focus on risk factors shared by chronic diseases in order to improve the periodontal health of Danish adults. Developing more effective approaches for prevention has been a permanent challenge for occupational health. A major obstacle to this goal has been the lack of communication and knowledge of problems affecting workers. Until recently, few studies had investigated the relationship between oral conditions and their impact on people’s lives; but in the last decade, there has been increased interest in quantifying the diseases. Various instruments were developed in an attempt to understand and assess how the oral problems have affected the daily lives of people. Open or structured interviews provide greater understanding of human behavior and people’s beliefs. The absence of predetermined interview responses offers the possibility of new perspective for social and cultural variables often judged by the researcher. In conclusion, taken together and considering the applied methodology, knowing the habits and the profile of the workers is a relevant factor to promote an oral health attention in the context of the occupational health. Gingival bleeding was found to be a strong indicator in workers’ selfperceived oral health and quality of life. References
Copyright © 2011 - Brazilian Journal of Oral Sciences The following images related to this document are available:Photo images[os11046f2.jpg] [os11046f1.jpg] [os11046t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}