 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 10, No. 4, Oct-Dec., 2011, pp. 236-240 Gunshot injuries in the maxillofacial region: a retrospective analysis and management Leandro Lauriti1, Sandra Kalil Bussadori2, Kristianne Porta Santos Fernandes3, Manoela Domingues Martins4, Raquel Agnelli Mesquita-Ferrari4, João Gualberto de Cerqueira Luz5
1Master’s Degree Student in Rehabilitation Sciences; Professor, Surgery Sector, Nove de Julho University, Brazil, 2 PhD Professor, Master’s Degree Program in Rehabilitation Sciences, Nove de Julho University, Brazil, 3PhD in Immunology; Professor, Master’s Degree Program in Rehabilitation Sciences, Nove de Julho University, Brazil, 4Professor, Master’s Degree Program in Rehabilitation Sciences, Nove de Julho University, Brazil, 5Professor, Surgery Sector, University of São Paulo, Brazil. Received: April 11, 2011 Code Number: os11048 Abstract
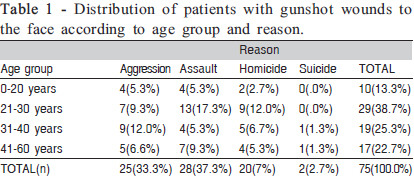
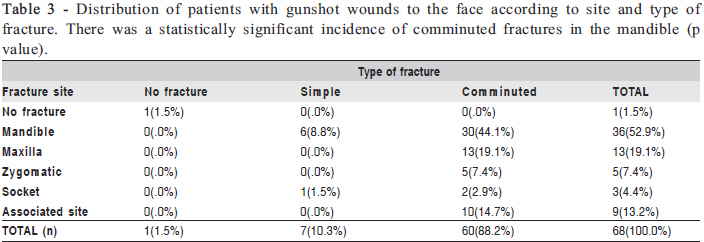
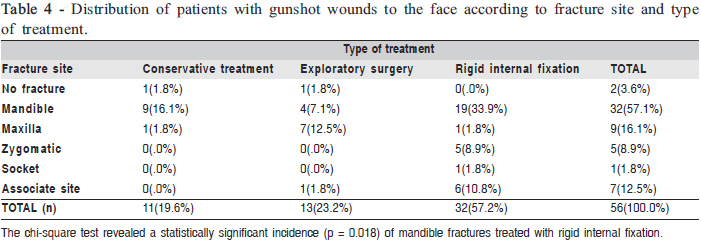
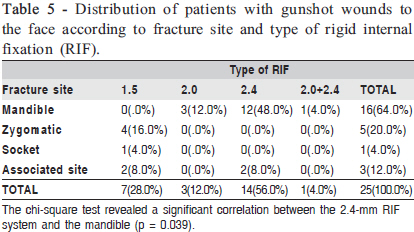
Aim: To analyze gunshot wounds to the face, assessing the characteristics, immediate treatment, late treatment, complications and after effects. Keywords: gunshot wounds, comminuted fractures, internal fixation of fractures. Introduction Gunshot wounds result from the transmission of kinetic energy from the bullet to the tissue with which it collides, with greater projectile speed leading to greater damage1-3 . The initial wound depends on the impact of the bullet, with the occurrence of an air pressure wave within two milliseconds that distends the tissue, forming a temporary spindle-like pulsating cavity fourfold larger than the bullet3-4 . The pulsation of the temporary cavity aspirates bacteria from the skin to its interior, characterizing an additional source of infection5 . To penetrate the skin, the bullet needs to be traveling at a velocity of 50 to 70 m/s, which causes abrasion to the dermis and epidermis. Axon degeneration occurs in the nerve tissue, giving rise to anesthesia, paresthesia and paralysis. The rigid bone is fragmented; fracture velocity of the bullet is 65 m/s2-4,6-7 . A study on ballistic impacts in the face established greater resistance to impacts to the frontal region (6.0 kN), whereas the mandible and zygomatic region are considerably more fragile (1.9 kN and 1.6 kN, respectively)8 . Knowledge on factors such as impact velocity, release rate of kinetic energy, retardant effect, bullet design, bullet mass, type of weapon and ballistic coefficient is essential to proper treatment6,9 . Clinically, patients having suffered gunshot injuries may exhibit signs of shock, neurological impairment, rapidly expanding hematoma and obstruction of the airways. Thus, immediate priority treatment is the control of bleeding and unblocking the airways2,10. In the face, tooth and bone fragments act as secondary projectiles, causing damage far from the original entry wound, which is difficult to diagnose11 . Analysis with both profile and anterior-posterior radiographs allows the adequate localization of projectiles11 . Therapeutic conduct regarding facial damage is based on the analysis of the projectile and the treatment of bone factures. The removal of the projectile is only indicated in cases of pain, functional limitation and signs of migration5,11-12. The treatment of comminuted fractures of the mandible by projectiles was once based on the use of Kirschner wire, which was believed to be viable treatment to avoid the displacement of the periosteum5. Rigid internal fixation (RIF) in comminuted fractures common in gunshot injuries is currently the conduct of choice, as it returns form and function with minimal complications and leads to the revasculation of the comminuted segments. Locking plates are the most indicated for comminuted fractures in the mandible due to the locking of the screw in the plate, which allows a space between the bone surface and plate, maintaining the perimeter of the arch 13-15 . The bone reconstruction period ranges from three to 12 months following the revitalization of the injured tissues and maturation of the scars2,5,9. The decisive factors for successful bone reconstruction are the severity of the injury, destruction of the soft tissue and degree of bone fragmentation. The donor area is determined by the degree of bone loss and age group; there is a preference for autogenous grafts from the iliac crest or ribs (costochondral) and free grafts from the fibula2,16-17. Costochondral grafts in the zone of traction and torsion forces, as in the symphysis, are contraindicated, as are thick grafts with little irrigation17-18. In cases of mandibular loss with the proximal and distal stump stabilized by the plate, the iliac crest is used. For young patients with loss of the distal stump, including the temporomandibular joint, a costochondral graft is indicated, whereas a free fibula graft is indicated for this type of loss in adults17 . With the increasing violence in urban centers, the number of victims of gunshot wounds has been on the rise. However, few studies have analyzed the characteristics and treatment conduct involved in such injuries. Thus, the aim of the present study was to retrospectively evaluate cases of gunshot wounds to the face in order to understand the clinical characteristics, treatment and complications in a Brazilian population. Materials and methods This study received approval from the local ethics committee under process nº 010/06. A retrospective observational study was carried out involving 75 cases of victims of gunshot wounds to the face treated at the Oral and Maxillofacial Traumatology Unit of the Dr. Arthur Ribeiro de Saboya Hospital in the city of São Paulo (Brazil) over an 8-year period. Information was collected from the charts of each patient, including demographic data, reason for the gunshot wound (aggression, assault, attempted homicide, attempted suicide), entry and exit wounds, clinical aspects and fracture site, considering three large areas of the face: zygomatic region, maxilla and mandible. Gunshot wounds in the mandible were subdivided into two groups: condyle, ramus or coronoid process (CRC) fractures and angle, body or symphysis (ABS) fractures. Data were also collected on the type of fracture, immediate conduct (such as procedures for the permeabilization of the upper airways, control of bleeding, suturing, debridement and surgical cleaning) and further conduct (conservative treatment, exploratory surgery and RIF) as well as complications and after effects. Data analysis involved the chi-square test, with the level of significance set at 5% (p<0.05). Results In the present sample, there was a predominance of the 21-to-30-year age group (38.7%) and the male gender (92%). The gunshot wounds were caused mainly by assaults (37.3%), followed by aggression (33.3%), attempted homicide (26.7%) and attempted suicide (2.7%) (Table 1). There was a predominance of entry wounds on the left side (58.5%) and exit wounds on the right side (53.7%). The most common clinical signs were pain, edema and trismus. With mandible fractures, paresthesia, increased salivation, malocclusion, bone exposure, deviation of mouth opening and premature contact were noted. When the zygomatic region was affected, otorrhagia, epistaxis, diplopia and paresthesia were noted. In maxillary fractures, oroantral and oronasal communication predominated. Of the 75 patients, 4 died and analyzed data from only 71 cases as shown in Table 2. The most affected sites were the mandible (50.7%), maxilla (18.3%), zygomatic region (7.0%) and eye socket (4.2%). There were associations between the maxilla and zygomatic region (4.2%), mandible and maxilla (2.8%), mandible and zygomatic region (2.8%), maxilla and eye socket (2.8%). Fractures in more than one site totaled nine cases (12.6%). The nose was affected in 1.4% of cases. No fractures occurred in 5.6% of cases. There was a statistically significant incidence of mandible fractures in the male gender (p = 0.003) (Table 2). Of the 71 patients evaluated, only 68 had completed their data records in full form, others were transferred to other services. A total of 88.2% of the patients had comminuted fractures (44.1% in the mandible), whereas 10.3% had simple fractures and 1.5% had no fractures. Associated sites (maxilla/ mandible, maxilla/zygomatic region, maxilla/nose, maxilla/ eye socket and mandible/zygomatic region) were grouped on a single line in Table 3. There was a statistically significant incidence (p value) of comminuted fractures in the mandible (Table 3). Of the 68 patients studied, 56 received some form oftreatment of our specialty as conservative treatment, surgical exploration or rigid internal fixation (RIF). The others were referred to other specialties such as neurology and orthopedics. RIF was the predominant type of treatment (57.2%), followed by exploratory surgery (23.2%) and conservative treatment (19.6%). The fractures occurred in the nasal region associated with the jaw line associate site grouped in Table 4. The chi-square test revealed a statistically significant incidence (p = 0.018) of mandible fractures treated with RIF (Table 4). Of the 56 patients evaluated for the type of treatment system and internal fixation used only 25 showed in their records the data specified. The 1.5-mm system predominated in the zygomatic region in 16% of cases. The system of rigid internal fixation on the face was the predominant 2.4mm used in 56.0% of cases. Among the cases in which the RIF system was used, there was predominance in the mandible (64.0%). The chi-square test revealed a significant correlation between the 2.4-mm RIF system and the mandible in 48.0 % of cases (p = 0.039) (Table 5). In the fractures that occurred in the mandible (ABS+CRC), RIF was the predominant treatment (61.8%), followed by conservative treatment (26.5%) and exploratory surgery (11.8%). Immediate complications occurred in 25% of the cases. The main complications were postoperative infection in the mandible, ear canal and eye socket in seven cases (9.3%). Paresis occurred in four patients (5.2%). Motor deficit of the facial nerve occurred in three cases (4%). Sinusitis occurred in two cases (2.6%). Soft tissue fibrosis and loss of substance occurred in two cases (2.6%). Optic nerve injury occurred in one case (1.3%). Among the 75 patients analyzed, there were 4 deaths (5.3%). After effects occurred in 11.7% of the cases. There were two cases of paresthesia (2.6%) – one in the infra-orbital nerve and one in the inferior alveolar nerve. Facial asymmetry occurred in two cases (2.6%). Dysphagia and speech difficulties occurred in two cases (2.6%). There was one case (1.3%) of paralysis stemming from an injury to the facial nerve. There was one case (1.3%) of a maxillary injury with subsequent formation of oronasal and oroantral fistula. There was one case (1.3%) of pseudo-arthrosis caused by loose osteosynthesis material. Discussion The individuals with gunshot wounds to the face in the present study exhibited different clinical characteristics and underwent different forms of treatment. With regard to gender and age group, the findings are in agreement with those reported in the literature, revealing a predominance of the male gender and young adults17-25. A retrospective study on gunshot wounds and explosions reports 1,155 injuries, 36% of which were gunshot wounds; the male gender was affected in 71% of the cases (84% of gunshot injuries); 53% of the sample was between 15 and 29 years of age (59% of whom received gunshot wounds); and there were greater proportions of open wounds (63%) and fractures (42%)5 . Interpersonal violence, alcohol, drugs and poverty have been reported as the main reasons for gunshot wounds24. In a study on gunshot wounds in children and adolescents between 0 and 19 years of age, the mortality rate was 19.7% and the main cause was assault (78.7%)26. In the present study, there was a predominance of assaults, followed by aggression and attempted homicide, which corroborates the findings reported by Cowey et al.27 . There was a predominance of entry wounds on the left side and exit wounds on the right side, configuring a piercing pattern for gunshot wounds to the face. This predominance of the left side suggests a connection with the assaults, and this side of the face exposed to the assaults on drivers likely. The face is a common site for gunshot wounds; a previous study reports a prevalence of 33.33% in the neck and face23 . In another retrospective study, entry wounds in the right temporal bone were prevalent20 . The sites most affected by gunshots in the present study were the mandible, maxilla and zygomatic region, which is in agreement with previous studies27. Other studies found a prevalence of gunshot wounds in the maxilla, followed by the mandible7. Hollier et al. retrospectively assessed 84 patients and found fractures mainly in the zygomatic region (34.52%), mandible (29.76%) and eye socket (26.19%)21 . Regarding mandible fractures, the angle, body and symphysis were the most affected sites. Similar data are reported by other authors12,27. Comminuted fractures predominated, which is in agreement with a review study13. The predominant treatment modality in the present study was RIF. Comminuted fractures lead to a preference for RIF due to the insufficient amount of bone to establish vectors of force13-15,28. In the present sample, RIF was the predominant form of treatment for gunshot wounds in the mandible, agreement with other studies19. However, a previous study reports the treatment of such wounds with maxillomandibular block and osteosynthesis with steel wire, with the use of RIF in the angle, body and symphysis of the mandible12 . Immediate complications occurred in 25% of the patients in the present study, four of which ended in death. A number of studies report that the complications that lead to the death of the patient are generally stroke, hypovolemia, sepsis, pneumonia, aneurism, osteomyelitis, abscesses and meningitis10,19. The cases of osteomyelitis were resolved with culture/antibiogram and specific antibiotic therapy followed by drainage. Tracheotomy and exploratory surgery of intracranial injuries are other immediate complications10,21,29. Ellis et al. report a significant correlation between the degree of comminuted fractures and the development of complications in a study on treatment methods for patients with comminuted fractures of the mandible over a 10-year period; 35.2% of those with more serious wounds treated with external fixation, 17.1% of those treated with maxillomandibular block and 10.3% of those treated with open reduction and RIF suffered complications13. However, the primary treatment of injuries to bone and soft tissues may be carried out at the time of debridement, thereby minimizing the rates of hospitalization, procedures and complications29 . One study on gunshot wounds to the mandible reports the following after effects: infection, deviation of mouth opening, malocclusion, bone loss and reduced motor activity16 . The treatment of the after effects resulting from gunshot wounds involves multidisciplinary therapy, with procedures such as rhinoplasty, blepharoplasty and orthognathic surgery7,21,30. For mandible reconstruction in adults having suffered gunshot wounds, osteogenic distraction causes the simultaneous expansion of the bone and soft tissues, thereby accelerating rehabilitation with bone-integrated implants30 . The present retrospective study found that males between 21 and 30 years of age were most affected by gunshot wounds to the face, with assaults as the main reason for the injuries. The entry wound was mainly on the left side and the exit wound was mainly on the right side of the face. The mandible was the most affected site and associated to comminuted fractures. Rigid internal fixation was the predominant form of treatment. Paresis, paralysis, infection, sinusitis and soft tissue fibrosis were the main immediate complications in the sample studied. The percentage of after effects was low and characterized by paresthesia, paralysis, oroantral and oronasal fistula, pseudo-arthrosis and loss of vision. References
Copyright © 2011 - Brazilian Journal of Oral Sciences The following images related to this document are available:Photo images[os11048t3.jpg] [os11048t4.jpg] [os11048t1.jpg] [os11048t5.jpg] [os11048t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}