 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 10, No. 4, Oct-Dec., 2011, pp. 241-245 Knowledge, attitude and practice on hepatitis B prevention among dental professionals in India R. Sudhakara Reddy1, L. A. Swapna2, T. Ramesh3, K. Pradeep4
1Professor and H.O.D, Department of Oral Medicine and Radiology, Vishnu Dental College, Bhimavaram, Andhra Pradesh 2Graduate student, Department of Oral Medicine and Radiology, Vishnu Dental College, Bhimavaram, Andhra Pradesh 3Associate professor, Department of Oral Medicine and Radiology, Vishnu Dental College, Bhimavaram, Andhra Pradesh 4Assistant Professor, Department of periodontics, Sri Sai College of Dental Sciences Vikarabad
Received: July 05, 2011 Code Number: os11049 Abstract
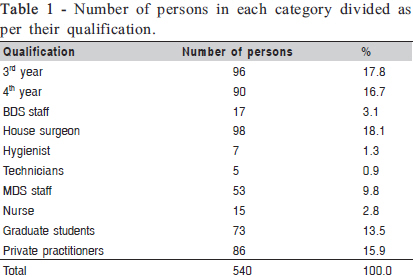
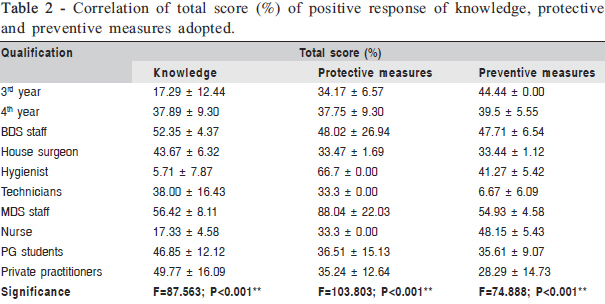
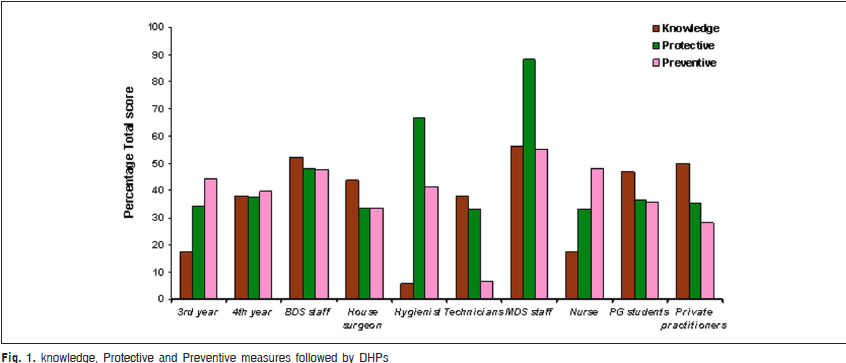
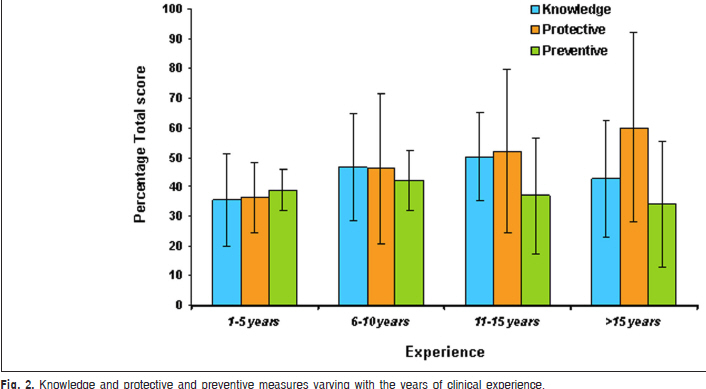
Aim: To obtain comprehensive information about the knowledge, attitude and practices towards hepatitis B infection by dental health care professionals, and their effort to prevent the transmission among the patients. Keywords: dental health care professionals, hepatitis-B, protective and preventive measures. Introduction Dental health care professionals are said to be at a risk of infections caused by various micro- organisms including M. tuberculosis, hepatitis B, hepatitis C viruses, streptococci, staphylococci, herpes simplex virus type 1, HIV, mumps, influenza, and rubella1-3. In a dental office, infections can be expedited through several routes, including direct contact with blood, oral fluids or other secretions; indirect contact with contaminated instruments, operatory equipment or environmental surroundings; or contact with airborne contaminants present in either droplet splatter or aerosols of oral and respiratory fluids4. Hepatitis-B Virus (HBV) is a major worldwide cause of acute and chronic liver infection, cirrhosis, and primary hepatocellular carcinoma. There are more than 300 millions carriers of the virus globally, and about 90% of these live in developing countries, among the World’s carriers, 75% are from the Asian continent, where between 8% and 15% of the population carries the virus5. The majority of the infections are sub-clinical, so that approximately 80% of all HBV infections are undiagnosed. It has been established that patient medical histories are unreliable in identifying exposure to HBV infection6. Regardless of the medical history, all patients should therefore be regarded as potential HBV carriers. Infection control practices in developing countries have not been widely indexed. Most of the hospitals have no infection control programmer due to indigence of awareness about the disease or penury of trained personnel’s. So a need exists for proper practice of infection control by both dental staff, dental nurses and hygienists6-9 . Center for disease control and prevention (CDC) has suggested the guidelines that include precautions and transmission based isolation safety measures that aid in safe working environment and eliminate the spread of infections9 . The aim of this study was to contrive comprehensive information about the knowledge, attitude and practice with regard to hepatitis B by dental health care professionals, and their effort to prevent the transmission of hepatitis among the patients. Materials and methods A cross sectional survey was conducted among 540 dental health care workers. A structured questionnaire was used to assess 3rd year and 4th year B.D.S. - bachelor of dental surgery students, house surgeons, graduate students, M.D.S. - Master of Dental Surgery, hygienists, medical lab technicians and nurses of Vishnu Dental College, Bhimavaram, Andhra Pradesh, India and local private dental practitioners in and around the state about the “methods to control cross infection, attitude towards protection and prevention of transmission of hepatitis infection , their approach towards sterilization of instruments and knowledge of immunization against hepatitis B virus. The questionnaire was designed and the ethical clearance was obtained from the ethical committee of Vishnu Dental College and Hospital, Bhimavaram. The questionnaire comprised of queries on knowledge, attitude towards protective and preventive measures with respect to hepatitis B vaccination and droplet isolation precautions as advocated by the CDC. The content authenticity was pretested on a random sample of population to ascertain practicability, cogency and rendition of responses. A visit was made to the faculty, students, lab technicians, hygienist and nurses of the dental college in Bhimavaram and the private dental practitioners in and around the state. The questionnaire was handed over with exigent instructions for the same. The data collected were maintained under strict confidentiality. Only valid responses were used for analysis. The age, sex and qualification & years of experience were also determined. Completed questionnaires were collected on the same day and prospectively analyzed. All responses were entered into a computer database and analyzed using a statistical package (SPSS; SPSS Inc., Chicago, Il, USA). Simple frequencies were calculated for all variables. All the frequency variables had percentages, cumulative percentages and corresponding related statistics. In the Knowledge questions having 10 questions , if given a response yes =1 and No=0, total maximum score will be 10, percentage of obtained score for each individual computed and compared according to age and other variables, Similarly protective and Preventive categories of questions were calculated. Descriptive statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean ± SD (Min-Max) and results on categorical measurements are presented in number (%). Significance level was set at 5 % level. Analysis of variance (ANOVA) was used to find the significance of study parameters between three or more groups of study subjects, Student’s t test (two tailed, independent) was used to find the significance of study parameters on continuous scale between two groups (inter-group analysis) on metric parameters. Results Out of the 540 respondents (Table 1), 53 individuals were MDS staff, 17 were BDS staff, 73 graduate students, 98 house surgeons, 186 were the students of 3rd and 4th year, 15 nurses,7 hygienists, 5 lab- technicians in the dental college and 86 private dental practitioners in and around the state of Andhra Pradesh. (Table 2) represents the percentage of responses on knowledge, attitude and practice regarding the protection and prevention of transmission of hepatitis-B infection. Mean score for knowledge of MDS staff was 56.42 ± 8.11; for protective measures was 88.04 ± 22.03; for attitude to prevent transmission was 54.93 ± 4.58 (Figure 1).Hygienists showed minimum knowledge with mean score of 5.71 ± 7.87, the protective and preventive measures followed were with a mean score of 66.7 ± 0.00 & 41.27 ± 5.42 respectively. None of them scored positive answer to the question -Have you attended any workshop regarding hepatitis transmission (or) prevention. Frequency of correct answer was higher for the question “Do you believe that hepatitis can transmit through saliva from patients?”, showing 81.3% positive response. Almost of 77.2% participants got the vaccination against hepatitis B. Only 14.4% thoroughly evaluated the patient to rule out any signs related to hepatitis. Nearly 65.9% of respondents were willing to perform any treatment procedures on patients known positive with hepatitis. As much as 53% of the dental health care professionals advised routinely for their patients to undergo blood investigations to rule out hepatitis before doing any invasive procedures. Under the category of questions relating to protective and preventive measures to avert transmission of hepatitis the results showed that about 89.8% of the participants responded that they change gloves for every patient. Only 15% of the individuals used protective eye wear for all procedures on patients or while assisting. 22.2% of the participants advise pre-procedural oral rinses (betadine/ chlorhexidine etc) to the patients. Only 1.1% participants used disposable kits for patients suspected or proved positive for hepatitis. And merely 2.2% of the participants used rubber dam where required to prevent atmospheric viral contamination. Though the knowledge of private dental practitioners was fair, their protective and preventive measures to avoid hepatitis transmission were not up to the mark, probably because of a small set up of clinics and other financial constraints. There was an increase in knowledge of dental health care professionals as their years of experience in dental clinic was increased from 1-5 years to 6-11 years (Figure 2). There was not much change in the knowledge, protective and preventive measures between dental health care professionals who had 6-11 and 11-15 years of experience. Discussion Though there is substantial literature regarding the knowledge and attitude of dentists towards other infectious diseases, no study assessed the different categories of dental health care professionals and their attitude towards hepatitis B infection and very few studies have been conducted in India in this regard. This study showed that B.D.S staff had a mean knowledge of 52.35, which was close to the knowledge showed by M.D.S staff (mean value of 56.42). However, the protective and preventive measures adopted by B.D.S staff (mean values of 48.02 and 47.71, respectively) was lower than the protective and preventive measures adopted by M.D.S staff (mean values of 88.04 and 54.93, respectively). Though the private practitioners showed a score of 49.77 as the mean value in knowledge, their measures followed to protect and prevent the transmission of Hepatitis was only 35.24 and 28.29 respectively. When the results were compared between the female and the male dental health care professionals, it was found that the female subjects were appropriately following the protective and preventive measures to avert the transmission of hepatitis. Several other similar studies have also been conducted to investigate the infection control knowledge, attitude and practice of dental health care professionals. Previous study among Nigerian investigators found that nearly 97.5% dentists routinely used gloves and 70.6% used face masks and 61.3% dentists reported to use protective gowns and eye wear during the procedures10. In our study, nearly up to 89.8% of the respondents changed their gloves for every patient and 81.1% of participants used protective clothing, but only 16.5% of participants used protective eye wear during procedures. Previously, the wearing of gloves before examining patients was hardly practiced regularly as an essential part of cross infection control. However, 25% of dental health care professionals in this study routinely wore gloves before patient examination. Whether routine wearing of gloves would prevent cross infection of blood borne viruses has not been resolutely established nevertheless, it would protect minor cuts, and abrasions from contamination and so reduce the transmission of HBV from carrier to practitioners10-13 . Only 20.2% practitioners in this study frequently scrubbed their hands with disinfectant before and after gloving, there is evidence of a reduction in skin flora when hands are scrubbed with soap and this should be encouraged in practice14-16 . Viral hepatitis caused by HBV is a disease that has no oral manifestation but is of great concern to the dental profession due to ease of transmission of the virus from patients with the condition. It may be difficult to identify those capable of transmitting HBV for several reasons. Many patients infected with hepatitis B virus may be unaware of their carrier status or they may be asymptomatic. Others may not want to disclose their infectious status10-12 . In a previous study, only 32% of the dentists took vaccination against hepatitis, where as 77.2% of the dental health care professionals in our study were vaccinated against hepatitis10. Similar study conducted to assess the hepatitis B awareness and attitudes among dental health care workers in Riyadh Saudi Arabia, results showed that nearly 43% did not have their antibody titre measured after completion of the full course to assess the efficacy of the vaccine. On the contrary, 87.9% of the dental health care professionals in our study did not check their antibody titre measured after completion of course of vaccination4. These findings are somewhat similar to those of several other Western-based studies in which post-vaccination testing had not been carried out in between 38-54% of dental health care professionals17-21 . Saheeb et al in a similar study found that nearly 19.5% of the dental health care professionals reused syringes, which was less when compared to our study where nearly 56.5% dental professionals reused syringes10 . Blood is very often found in the aerosols produced by dental equipment like an ultrasonic scaler or other highspeed equipment Ultrasonic scaling was obviously associated with increased air contamination levels confirming the results reported by several other studies showing that this procedure is the main executor of airborne contaminants in dentistry. Previous research demonstrated that rinsing with an antiseptic mouthwash produced a 94.1% reduction in airborne contaminants compared to the non-rinsed controls. Hence, high volume suction evacuators and preprocedural oral rinses would prevent the air contamination22-25 . A survey was conducted to assess the extent of awareness regarding transmission of Hepatitis among the DHPs in Bhimavaram, Andhra Pradesh, India. This study also threw light on the knowledge, attitude and behavior of dental health care professionals regarding the protective and preventive measures to avert the transmission of hepatitis B, and also made them seriously think about the risks that their patients and they themselves face during the treatment procedures. As we approached the participants to collect the filled questionnaire, the respondents were curious to know the correct protocol to follow during the dental treatment procedures to prevent the transmission of hepatitis infection and the information about the vaccination against hepatitis and its importance. One of the limitations of this study was that we could not supervise the respondent’s practice, so we had to rely on their subjective self-assessment. Therefore, the responses might not have accurately reflected the true levels of knowledge, attitude and behavior, and thus, the reported level of practice might be lower than the real level. It is important for any hospital or a dental clinic to set up CDC protocol to prevent the spread of infectious and transmissible diseases. For this purpose, it is important that the dental health care professionals be aware of the risks and the seriousness of infections. Educational programs on infection control isolation precautions for all the health care workers, especially the dental health care professionals, and the facilities to allow compliance with the infection policies are necessary to lessen the infection hazards among dental health care professionals and their patients. Acknowledgements We wish to thank all the participants who took part in our study. References
Copyright © 2011 - Brazilian Journal of Oral Sciences The following images related to this document are available:Photo images[os11049t1.jpg] [os11049t2.jpg] [os11049f1.jpg] [os11049f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}