 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Surgical dental treatment prior to liver transplantation Paulo Sérgio da Silva Santos1, Maria Izabel Sarmento e Souza Pacheco2, Mateus Pereira Alonso Soler3, Valtuir Barbosa Felix4
1DDS, MD, PhD, Department of Stomatology, Bauru School of Dentistry, University of São Paulo, Brazil, 2DDS, Department of Oral and Maxillofacial Surgery, Santa Casa de Misericórdia of São Paulo, São Paulo, Brazil, 3DDS, Department of Oral and Maxillofacial Surgery, Hospital Regional Sul, São Paulo, Brazil, 4DDS, MD, PhD, Department of Oral and Maxillofacial Surgery, Hospital Regional of Osasco, São Paulo, Brazil Received: May 26, 2011 Code Number: os11052 Abstract
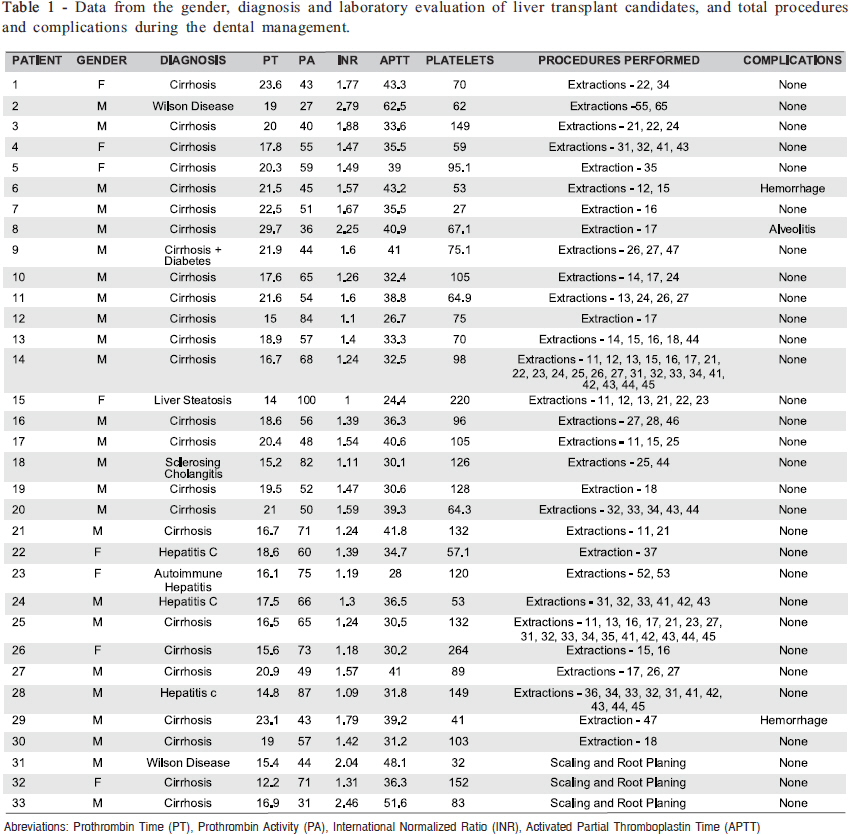
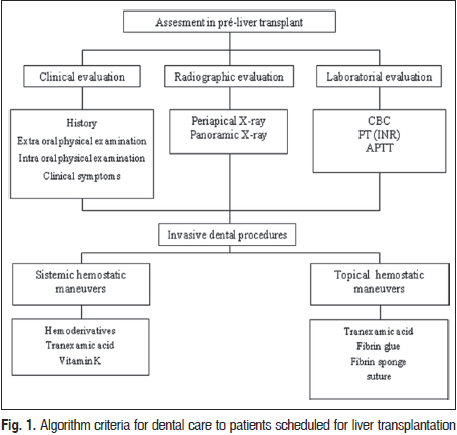
Oral-source infections are a potential threat for transplant candidates because oral diseases tend to be more severe and untreated in people who have received transplants. Although not yet scientifically proven, evaluation and dental treatment during the pre-transplantation period is recommended in order to prevent infections and resultant odontogenic-origin sepsis during the post-transplant period, when patients receive immunosuppressive therapy. Keywords: surgery, oral, hemostatic techniques, organ transplantation. Introduction Dental treatment, including the elimination of oral and mucosal infection foci, is essential for transplant patients during both preparation and post-surgery periods; patients should be under constant dental care and undergo mycological tests, especially in the first months1-5 . Oral-source infections are a potential threat to transplant candidates because oral diseases tend to be more severe if left untreated in people who have received transplants3,6 . Although no evidence-based guidelines for dental septic focal treatment exist, patients should be advised to have dental foci removed before undergoing organ transplants in order to avoid post-transplant systemic and local oral complications. In addition, these patients should be organized into a dental or oral maxillofacial surgical follow-up program7 . Teeth that need to be restored but are impossible to treat, as well as those with advanced periodontal disease, must be extracted. Non-vital teeth (at risk of infection) must be extracted or endodontically treated, and all active caries lesions should be treated and resulting cavities should be restored8. For any type of oral surgery, the patient must have an intact hemostatic process because even the least invasive procedures can lead to severe bleeding, increased risk of infection, poor wound healing and airways may be compromised if there is bleeding in critical fascial spaces9 . Any liver disease that affects the synthesis of clotting factors may manifest itself by an increase of prothrombin time (PT), which reflects the extrinsic pathway for the coagulation mechanism. The activated partial thromboplastin time (APTT) reflects all clotting factors except platelet factor III and factors XIII and VII and is indicative of the function of the coagulation mechanism’s intrinsic pathway. Therefore, before any surgical procedure, the preoperative evaluation of these patients must include a complete blood count (CBC), PT, international normalized ratio (INR) and APTT9. This research aimed at evaluating invasive dental procedures for removing dental foci in patients scheduled for liver transplantation along with any accompanying complications. Material and methods After approval by the Research Ethics Committee for the Santa Casa de Misericórdia de São Paulo, this study evaluated 33 prospective patients who were candidates for liver transplants and had been receiving treatment in a dentistry department for patients with special needs, during 3 years, according to the indication/medical records maintained by the liver transplant team. All potential candidates in the liver transplant program from regional Hospital of São Paulo, Brazil, during this period were included in the study. The 33 selected patients consisted of 25 (75.8%) males and 8 (24.2%) females, with a mean age of 53.15 years. They underwent clinical, radiographic (panoramic and periapical x-rays) and laboratory (CBC, PT/INR, APTT) examinations for diagnosis and planning of dental treatment, totalizing 50 procedures. Tooth extraction criteria were: presence of residual roots; extensive carious lesions with partial crown destruction and risk of pulpal involvement; teeth with periapical lesions; semi-erupted teeth; teeth with periodontal involvement; as well as the capacity and interest of the patient in caring for and maintaining oral hygiene. The periodontal treatment consisted of scaling and root planing divided into several sections, starting from the supra-gingival area, gingival and subgingival level for cases of mild to moderate periodontitis, and prescription of 5% tranexamic acid mouthwash three times a day during 7 days. Patients were subjected to oral surgery for dental extraction to remove odontogenic foci, and received systemic antifibrinolytic therapy according to laboratory parameters INR > 3.0, APTT> 60 sec and platelet count <30,000 cells/µL). Local hemostasis techniques, applied to all patients, consisted of: application of a tranexamic acid paste (macerated pill mixed with saline or anesthetic solution) in order to fill the alveolar socket after dental extractions; the placement of fibrin sponge that was properly trimmed and well adapted to the alveolar socket10; suture with maximum coaptation of the gingival edge and application of another layer of tranexamic acid paste applied to the wound11. The systemic hemostasis technique consisted of the administration of blood derivate or tranexamic acid12 (500 mg, 3 times day), starting 2 days before the procedure and ending 3 days after. Results Fifty invasive dental procedures were carried out on the 33 patients. Three of them were subjected to basic periodontal treatment and 47 were subjected to multiple (2 or more teeth, n = 39) or single (1 tooth, n = 8) extractions. Three invasive procedures resulted in postoperative complications: 1 (3.03%) single post-extraction infectious alveolitis and 2 (6.06%) cases of postoperative bleeding as a result of a simple extraction and a multiple extraction (Table 1). Evidence of poor oral hygiene in this group of patients was clearly demonstrated by the number of tooth extractions needed. All patients had altered laboratory results (CBC – platelet count, PT/INR, APTT/RT), consistent with the clinical status of end-stage liver disease. The only infectious complication was a dry socket, which was treated by removing sutures, intra-alveolar curettage and application of zinc oxide and eugenol paste13. The hemorrhagic complications were treated by removal of sutures, intra-alveolar curettage, irrigation with saline and 2% chlorhexidine, application of tranexamic acid paste in the alveolar socket, fibrin sponge placement, suture, application of another layer of tranexamic acid paste and daily monitoring within the first 72 h postsurgery. Discussion Although there are no evidence-based guidelines for dental septic focal treatment, patients should be advised to have their dental foci removed before undergoing organ transplants and receiving immunosuppressive therapy. Meticulous clinical examination, including extraoral and intraoral, and radiographic examinations (panoramic and periapical x-rays) are important to find infectious foci and to establish the diagnosis and the development of an adequate treatment plan. These examinations are all part of the protocol for pre-organ-transplant dental evaluation. Laboratory assessment before dental surgery, which includes blood cell count, PT, APTT and platelet count, is mandatory for assessing the risk of bleeding during surgery or in the postoperative period, and provides the dentist and the medical team with guidance parameters that will demonstrate if there is risk of surgical or clinical complications during the monitoring of this group of patients (Figure 1). The patients in this study sample had poor oral conditions, with the presence of plaque and calculus, periodontitis, extensive carious lesions, residual roots infection by Candida and xerostomia. Radiographic examination revealed periapical lesions, unerupted teeth, and alveolar ridge resorption due to periodontitis. These clinical and radiographic findings are consistent with our research findings, which show that liver disease patients are in large part, consumers of alcohol and tobacco, and have poor oral hygiene5,14 . Strategies for improving the preventive dental care are needed15 for this group and the role of the multidisciplinary team is essential16 . In this study sample, despite the significantly altered laboratory tests and surgical procedures carried out, the rate of complications after dental surgical procedures in the liver transplant candidates (6.06%) was lower than that found by Niederhagen et al. (2003)17 (15.4%) and fairly consistent with that found by Stanca et al. (2010)18 (5%). The few complications were of hemorrhagic and infectious nature and were easily controlled. Our results suggest that proper surgical techniques associated with local and systemic haemostatic procedures are effective in preventing complications associated with coagulation disorders that liver disease patients may develop. Of the 33 patients in this study, 2 had previously received blood transfusions, and 31 patients were treated only with local hemostatic maneuvers. In two cases, when bleeding during surgery was greater than expected, a successful intravenous administration of vitamin K was carried out. The reduction in salivary flow and the presence of candidiasis found in some patients may be associated with the use of diuretics for the treatment of ascites and edema, frequent complications of cirrhosis, which increases the deposition and retention of plaque as well as the susceptibility of opportunistic infections. This condition requires special attention from the dental professional to prevent and treat opportunistic infections. Solid organ transplant patients have a high risk of developing squamous cell carcinoma of the upper digestive tract, which is also associated with prolonged use of immunosuppressant drugs, but it is primarily attributed to smoking5. This condition requires special care when monitoring these patients in the post-transplant period. Most patients in this study reported not having received any dental monitoring because dental professionals reported lack of knowledge on management techniques and treatment of liver disease and transplant patients. This fact corroborates the findings of Guggenheimer et al. (2007)4, who studied patients undergoing liver transplant5. The need for radical prophylactic dental sanitation should be further studied so that appropriate protocols are established for these patients. In conclusion, the surgical intervention to remove dental foci in liver disease patients requires careful clinical evaluation, laboratory tests, knowledge and skills in the use of local and systemic hemostatic maneuvers, and a well established partnership approach between dentists and physicians in order to maintain a low risk of complications. Acknowledgements We thank the Santa Casa de Misericórdia de São Paulo for the assistance given to us throughout our research. References
Copyright © 2011 - Brazilian Journal of Oral Sciences The following images related to this document are available:Photo images[os11052t1.jpg] [os11052f1.jpg] |
| |||||||||

{kind=link}
{kind=link}