 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 10, No. 4, Oct-Dec., 2011, pp. 262-267 Effect of light-curing units on gap formation and microleakage of class II composite restorations Giovana Mongruel Gomes1 , Bruna Fortes Bittencourt1 , Gibson L. Pilatti2 , João Carlos Gomes3, Osnara Maria Mongruel Gomes3 , Abraham Lincoln Calixto3
1DDS, MS, PhD student, Department of Restorative Dentistry, School of Dentistry, State University of Ponta Grossa, Brazil 2DDS, MS, PhD, Professor, Department of Periodontology, School of Dentistry, State University of Ponta Grossa, Brazil 3DDS, MS, PhD, Professor, Department of Restorative Dentistry, School of Dentistry, State University of Ponta Grossa, Brazil
Received: August 01, 2011 Code Number: os11054 Abstract
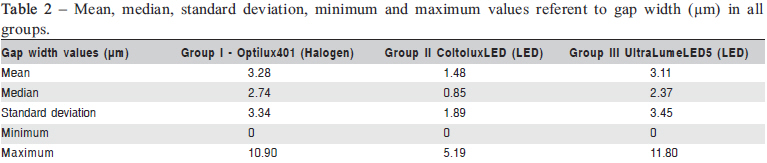
Aim: This in vitro study evaluated gap width formation and marginal microleakage in Class II composite restorations light-cured with three different light-curing units. Keywords: composite resins, dental curing lights, polymerization. Introduction Light-cured composite remains in focus since its introduction in Dentistry in the 1960’s1. Its importance is due to several factors, among which aesthetics is considered essential. However, the adhesion between composite resin and dental tissues remains a challenge for dental practice after all these years2-5 . Resin-based materials have an inherent characteristic, which is due to the polymerization of monomers to polymers1. When this strength exceeds the adhesive bond strength to cavity walls, marginal gaps may appear between restoration and tooth6-7, predisposing the restoration to marginal infiltration8. A range of undesirable effects that include penetration of bacteria and oral fluids can result in staining, recurrent caries, postoperative sensitivity and ultimately irreversible pulp pathologies2, thereby decreasing the longevity of the restoration2,9. Several techniques have been proposed to reverse the problems caused by polymerization shrinkage of resin, including the use of an adhesive layer with sufficient bond strength and elasticity modulus to withstand the stresses transmitted to this interface10-11, as well as the use of the so-called lowshrink composites currently available in the dental market12-16 . The complexity of the factors that determine the stress generated by polymerization shrinkage is so great, that it could also be cited other contributing factors: cavity configuration1718, placement technique8,17, radiant exposure (dose)19, curing techniques17-18,20 and inherent properties of resin-based materials, such as the amount of filler load12,17-21. It is known that resin composite restorations with enamel margins have higher bond strength values than those with margins located in dentin, because this substrate is more critic22 . Among different light-curing units (LCUs) developed for photoactivation of resin-based materials, quartz-tungsten halogen (QTH) lamps and light-emitting diodes (LEDs) are still the most common devices. These LCUs emit blue light close to the absorption spectrum of camphorquinone (468 nm), the most common photoinitiator in resin-based materials23. Despite their popularity, halogen lamps have some disadvantages, such as accelerated degradation of the internal components, due to overheat generated by the lamp, requiring frequent replacement. LEDs are smaller, cordless and do not require filters. There is no heat output, so a cooling fan is not needed. However, they cost more than conventional halogen lamps and their battery must be recharged24. Studies have showed the LCUs may interfere on staining susceptibility and conversion degree of composites25, as well as in the amount of residual monomers found in adhesives26 . On the other hand, the literature has reported no significant differences on the color stability27, conversion degree28 and surface energy of various composite resins after curing by LED or halogen devices29 . Several studies have compared microleakage and gap formation in Class II composite restorations and the influence of different LCUs17,22,30-31, but with no consensus between the authors. Gap formation and leakage studies have been used as in vitro indicators of both retention and marginal sealing abilities of composite restorations22. Thus, the objective of this study was to evaluated gap formation and microleakage of Class II composite restorations light-cured with three different LCUs (one halogen lamp and two LED units). The null hypothesis tested was that LCUs do not influence gap formation or microleakage of Class II composite restorations. Material and methods Specimen preparation and restorative procedures This study was approved by the Ethics Committee (COEP) of the State University of Ponta Grossa – UEPG, under the reports number 08/2005 (microleakage analysis) and 09/2005 (gap measurement) and protocols number 01211/ 05 and 01212/05, respectively. Thirty-six sound human third molars extracted for orthodontic reasons, with no defects, were selected for this study. Immediately after extraction they were hand scaled to remove tissue remnants and stored in distilled water at 4 ºC and used for no longer than 6 months after extraction32 . Two Class II cavities were made in each tooth – one on each proximal surface – totalizing 72 cavities. All cavities were prepared as vertical slots, with the cervical margin in cementum, using a diamond bur #4137 (KG Sorensen, Barueri, SP, Brazil) mounted in a mechanical device (El Quip, São Carlos, SP, Brazil) that allowed standardized preparation of cavities with the following dimensions: 4 mm oclusal-cervical length, 1.8 mm buccolingual width and 2.1 mm cervical-axial depth. A new bur was used after five preparations. Teeth were randomly divided in three groups (12 teeth/group, totalized 24 restorations/group) according to the LCU used: Group I: halogen - Optilux 401 (Kerr/ Demetron Res. Corp., Orange, CA, USA); Group II: LED – Coltolux (Coltène Whaledent, Altstatten, Switzerland) and Group III: LED – UltraLume LED 5 (Ultradent, South Jordan, UT, USA). Table 1 shows more details concerning the LCUs used in the study. All cavities were restored with the same adhesive system (Adper Single Bond, 3M ESPE, St. Paul, MN, USA) and composite resin (Filtek P60, 3M ESPE). The composite resin was inserted according to the oblique technique, in increments of 2 mm, using a photocondenser tip (TDV Dental Ltda, Pomerode, SC, Brazil). Each increment was light-cured for 40 s, using the tested LCUs. The length of the photocondenser tip served as a guide to standardize the distance of the LCU from the restoration. After 24 h of water storage at 37ºC, the restorations were finished and polished with Sof-Lex discs (3M ESPE) according to the manufacturer’s instructions. Specimens were then subjected to a thermal cycling regimen of 500 cycles (5ºC ± 2ºC and 55ºC ± 2ºC), with a 15-s dwell time in each bath. The 36 teeth were bisected in a buccolingual direction with a water-cooled diamond saw (Isomet 1000, Buehler, Lake Bluff, IL, USA) to obtain mesial and distal halves, each one with a restoration, totalizing 72 restorations. Then, each half was sectioned longitudinally in the middle of the restorations, in such a way that each half produced two hemi-sections: one buccal and one lingual. Gap measurement Eighteen teeth were taken to a vacuum desiccator and sputter coated with gold-palladium (Polaron SC7620, Quorum Technologies Ltd., East Sussex, UK) for 5 min at 10 mA. Each specimen was examined by a scanning electron microscope (JSM 6360LV, Jeol Ltd., Tokyo, Japan) at a 15kV accelerating voltage at ×1000 magnification and SEM micrographs were taken for evaluation of gap width (µm) (Figure 1). Microleakage analysis The 18 teeth were used to evaluate dye penetration at the gingival wall of each specimen. Specimens were coated with two layers of nail varnish, and then exposed to 50% silver nitrate solution (Vetec Química Fina, Xerém, RJ, Brazil) for 2 h, photodeveloped (Kodak, Eastman Kodak Company, Rochester, NY, USA) for 16 h. Afterwards, teeth were washed with tap water and nail varnish layers were removed with the aid of manual cutting instruments. The teeth were sectioned in the same manner as previously described, and the microleakage was evaluated by two examiners using optical stereomicroscope (Olympus BX41, Tokyo, Japan) at ×40 magnification. Leakage was scored using the following criteria: 1, no dye penetration; 2, dye penetration extending up to 1/2 of cervical wall; 3, dye penetration extending to cervical wall, but without reach the axial wall; 4, dye penetration extending to cervical wall, reaching axial wall. If examiners disagreed, a forced consensus was reached and the consensus score recorded. Statistical analysis After measurements, as data did not confirm to the presuppositions of parametric analysis, the non-parametric Kruskal-Wallis test was used to compare the effect of each LCU on gap formation and marginal microleakage at a 5% significance level. Results Gap measurement Table 2 summarizes the results (mean, median, standard deviation, minimum and maximum values) for gap formation in the experimental groups. The first null hypothesis was accepted because there were no statistically significant differences (p=0.25) among the groups with respect to gap width. Marginal microleakage The frequencies of marginal microleakage scores are presented in Table 3. The second null hypothesis was also accepted because, although Group I showed lower microleakage scores follow by Group III and Group II, there were no statistically significant differences (p=0.072) among the experimental groups with respect to marginal microleakage. Discussion The polymerization reaction of resin-based composites involves the conversion of C=C bonds in individual monomer molecules and the formation of C-C bonds to form polymer chains, causing volume reduction, as covalent bonds are created and molecular distances and free volume are reduced33 . Light-activated composite resins start the polymerization process through the absorption of light by the initiator (usually a diketone), which once activated, reacts with a reducing agent (aliphatic amine) to produce radicals that bind the monomer molecule, making it active. The unsaturated monomer link opens, and subsequently acts on the other molecules from the monomer, forming a crosslinked macromolecule. In this polymerization process, generally there are three stages: Initiation, propagation and termination. In the first stage, photons of light energy at a wavelength around 450 nm to 500 nm, activate the initiator. The initiator depends on a co-initiator for the electron transfer and the formation of free radicals. The co-initiator usually is a tertiary amine that does not absorb light, but interacts with the camphorquinone when it is excited. Free radical is a highly energetic molecule with an unpaired electron. It needs to form a covalent bond with another compound, which, in turn, may be the double bond (C=C) present in the monomers. Propagation is the stage when the free radical reacts with the first monomer unit (C=C). The formation of a radical-monomer complex occurs, which aim to produce more connections with other monomers. In other words, it is a chain reaction with rapid growth of radical-monomer complex, forming a three-dimensional network, until the polymer formation. Termination is when two macroradicals collide, or when the active extremities of two chains that propagate react with each other and bind in a bimolecular reaction to form a single molecule no more reactive, ending the chain growth34 . The development of contraction stress of composites depends, among other factors, on the composition of the material (type of monomer, filler load, and their interaction), and factors related to resin composite polymerization (conversion degree, curing technique, placement technique, C-factor, and others)35. Regarding the composition of the material, Filtek P60 contains 61% of filler content (in volume) -silica and zirconia fillers with mean size of 0.6 µm - and a polymeric matrix consisting of Bis-GMA, Bis-EMA, UDMA and TEGDMA. As any resin-based composite, this material undergoes polymerization shrinkage. In the present study, it was used an only type of composite, since the objective was to verify the effect of different LCUs on gap formation and marginal microleakage. Variation between resin composites were excluded, as each material could have different compositions and, consequently, distinct degrees of polymerization shrinkage. The photoinitiator of Filtek P60 composite resin is camphorquinone (maximum absorption spectrum at 468 nm), and all the LCUs used in the present study work within this spectrum. It was also employed a device for standardization of the Class II cavities in order to avoid variations in their dimensions. Each LCU has its own wavelength specifications, advantages, disadvantages, and curing efficiency. It has been observed that scattering is greater with the halogen units36 . Also, LED units has more spectral purity than halogen lamps, as it has a narrow band of light emission with a wavelength between 450-490 nm, with peak emission at 470 nm, and this is the coincident blue light band with the absorption spectrum of most of the photoinitiators included in the composite resins, which allows full use of LEDs37 . The type of photoinitiator in resin-based materials significantly influences the curing efficiency of the material across the width of a restoration38. It also determines the most appropriate LCU to cure a particular type of composite resin, as the wavelength emitted by a LCU should match the absorption spectrum or absorption peak of the photoinitiator in that composite. Camphorquinone can be readily cured with halogen lamps and other units, but other photoinitiators (PPD, Lucirin TPO) pose a great problem because most commercially available LCUs do not match their spectrum24 . Another factor that affects light-curing efficiency is the filler particles of resin-based materials. These filler particles tend to scatter the light, and both filler content and size influence the light dispersion24. Smaller filler particles (0.1 µm to 1.0 µm) have maximal scattering because these particle sizes correspond to the wavelength range of the photoinitiator. Microfilled composites with smaller or greater particles scatter more light than microhybrid resins. If the refractive indices of the matrix and filler particles have an increased difference, light scattering is also increased. Therefore, the size and concentration of filler particles should be controlled depending on the refractive indices of the filler and resin matrix, as it also influences the resin color39 . The results of this study demonstrate that all groups showed gap formation. Corroborating these results, other studies have previously reported that all groups, regardless of the composite material12,16,21 or the curing technique22,40 were free of marginal gaps at tooth/restoration interface. The results of this study are supported by the literature. Researchers30-31,41 have found no differences in microleakage when LEDs or halogen lamps were used to photo-activate class II composite restorations. Small (2001)41 stated that although many improvements have been made, any material or method can ensure the effectiveness of the restoration if certain principles are respected, while another study30 found better overall results when 2nd generation LEDs and halogen lamps are used compared with 1st generation LEDs. On the other hand, differently from this study, Fernandes et al. (2002)42 reported that the use of LED units contributes to a better interface integrity, which is an extremely essential factor in procedures that utilize light-curing materials. Studies have found that using a LED20 or a halogen lamp18 in soft start mode reduces polymerization shrinkage and microleakage. All the discrepancies between these studies probably occur due to the different experimental designs of each study, especially the cavity size, polymerization method22, light intensity of LCUs and energy density per increment. Accurate knowledge of the polymerization process and control techniques may also contribute to the clinical performance of the restorative procedure and better marginal adaptation, hence, decreasing marginal gap formation17 . It is important to emphasize that this in vitro study used different LCUs with the same curing time (according to the manufacturer’s instructions), with no influence of other factors, such as energy density or power intensity. It is also known that the stress caused by polymerization shrinkage of composites has a multifactorial nature7. Therefore, select an appropriate restorative material, follow correct handling and placement techniques and use an appropriate LCU may allow for controlling polymerization shrinkage and having more aesthetic and durable Class II restorations due to reduction of marginal discoloration, recurrent caries and postoperative sensitivity17 . Within the limitations of this in vitro study, it may be concluded that there were no differences among the LCUs tested with respect to gap formation and marginal microleakage of Class II composite restorations. Further studies should be done to verify the interaction between the different factors that characterize gap formation and marginal microleakage, as well as ensure a better marginal adaptation at tooth/restoration interface. References
Copyright © 2011 - Brazilian Journal of Oral Sciences The following images related to this document are available:Photo images[os11054t2.jpg] [os11054f1.jpg] [os11054t1.jpg] [os11054t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}