 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Comparison of the centering ability of the ProTaper Universal, ProFile and Twisted File Rotary Systems Daniela de Andrade Mendes1, Carlos Menezes Aguiar2, Andréa Cruz Câmara3
1BDS, MSc student in Integrated Clinical Dentistry, Department of Prosthodontics and Oral and Facial Surgery, Dental School, Federal University of Pernambuco, Brazil, 2BDS, MSc, AssociateProfessor, Department of Prosthodontics and Oral and Facial Surgery, Dental School, Federal University of Pernambuco, Brazil, 3BDS, MSc, PhD, Department of Prosthodontics and Oral and Facial Surgery, Dental School, Federal University of Pernambuco, Brazil Received for publication: September 26, 2011 Code Number: os11058 Abstract
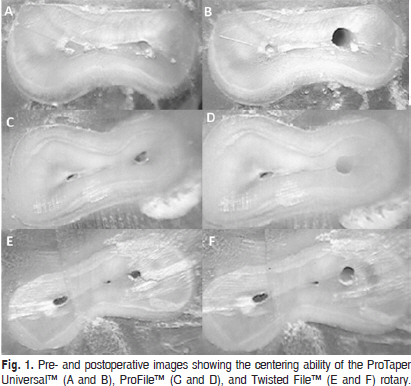
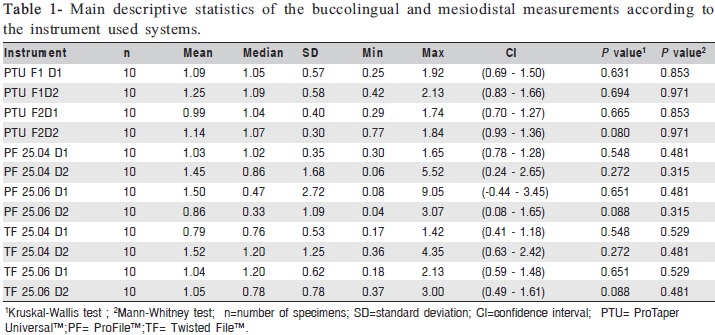
Aim: To determine the centering ability of Twisted File™ rotary system compared with ProTaper Universal™ and ProFile™ rotary systems by evaluating pre- and postoperative cross-sectional images of the apical root canals third. Keywords: instruments, ProTaper Universal, root canal, root canal preparation, Twisted File. Introduction Root canal preparation is one of the major components of endodontic treatment, and it is directly related to subsequent disinfection and filling1. The aim of root canal preparation is to form a continuously tapered shape with the smallest diameter at the apical foramen and the largest at the orifice to allow effective irrigation and filling2 without deviating from the original trajectory3-4. When curvature is present, endodontic preparation becomes more difficult, and there is a tendency for all preparation techniques to divert the prepared canal away from the original axis5. Nickel-titanium (NiTi) rotary instruments, due to their superelastic behavior and shape-memory properties, are able to maintain the original canal shape without significant transportation or creation of irregularities such as zipping, ledges, perforations, or danger zones, in curved canals6-7. Many types of rotary root canal instruments have been introduced, varying in cross-section, blade and pitch design, and taper8-10. The ProFile™ (Dentsply, Maillefer, Ballaigues, Switzerland) rotary system is a three-fluted file of constant taper, with three radial lands, a U-shaped cross-section, and noncutting safety tip11. The ProTaper™ NiTi rotary system has been upgraded to the ProTaper Universal™ system, which includes shaping, finishing, and retreating instruments. It incorporates a shallow, U-shaped groove at each of its convex triangular sides in cross-section, supposedly to improve flexibility in the larger instruments1,12-14. Recently, a completely different manufacturing process has been developed by SybronEndo to create a new rotary file for root canal preparation called the Twisted File™ (SybronEndo, Orange, CA, USA). These files have a triangular cross section with constant tapers of .04, .06, .08, .10, and .12. They are available in five tip sizes from 25 to 50. The manufacturer claims that the three new manufacturing processes of these files, namely R-phase heat treatment, twisting of the metal, and special surface conditioning, significantly increase the instrument’s resistance to cyclic fatigue and flexibility, even with .06-, .08-, .10-, and .12tapered instruments, maintaining the original canal center and minimizing canal transportation even in severely curved root canals5,15-17. There have been few studies published on the ability of the Twisted File™ rotary systems to maintain root canal morphology. By evaluating pre- and postoperative crosssectional images of the apical third of root canals, the present study set out to determine the centering ability of the Twisted File™ rotary system compared with the ProTaper Universal™, and ProFile™ systems. Material and methods Selection and preparation of the samples Thirty mesiobuccal canals of extracted human mandibular first molars (length, 20-21 mm) obtained from the Human Tooth Bank of the Department of Prosthodontics and Oral and Facial Surgery of the Federal University of Pernambuco, Brazil, were selected with the approval of the Ethics Committee of the Center of Health Sciences of the same University. The mesiobuccal roots had completely formed apices and severely curved root canals whose curvature ranged from 50° to 60° according to the canal access angle (CAA) technique18. After coronal access, the distal root was separated from the mesial root with a carborundum disk (KG Sorensen, Barueri, Brazil). The distal root was returned to the tooth bank, and the mesial root was washed in running water for 2 min and left to dry at room temperature. A #10 Senseus-Flexofile (Dentsply/Maillefer) was inserted into the mesiobuccal canal until its tip was visible at the apical foramen and the working length (WL) was calculated to be 1 mm less than the length obtained with this initial file. Obtaining the preoperative images The specimens were embedded in autopolymerizing resin acrylic blocks (Artigos Odontológicos Clássico Ltda., São Paulo, SP, Brazil) according to a previously described method3. After polymerization, the acrylic blocks were removed from the molds and sectioned transversely 3 mm from the apex for standardization purposes with the aid of a double-faced diamond disk (KG Sorensen). Preoperative images of the apical thirds were viewed with a ×10 stereoscopic magnifier (Ramsor, São Paulo, SP, Brazil) at the Biomaterials Clinical Research Unit of the Federal University of Pernambuco and captured digitally. The specimens were remounted in their molds and biomechanical preparation was performed. Biomechanical root canals preparation The specimens were randomly divided into three groups with 10 root canals each. All instrumentation was performed according to each manufacturer’s instructions. Random distribution of the groups considered the degree of canal curvature, allowing the average curvature, as well as the more severe cases, to be evenly allocated to each group: Group 1: ProTaper Universal™ Rotary System. The canals were instrumented at a rotational speed of 300 rpm (Driller Endo-Pro Torque, Sao Paulo, Brazil) as follows: (a) the SX file was used to one half the of the WL, (b) the S1 file was used up to 4 mm short of the apex, (c) the S1 and S2 files were used to the full WL, and (d) the F1 and F2 files were used to the full WL. Group 2: ProFile™ Rotary System. The canals were instrumented at a rotational speed of 300 rpm as follows: (a) #20.08 and #25.08 files were used up to the coronal one third of the root canal; (b) #20.06 and #25.06 files were used up to 4 mm short of the apex; and (c) #20.04, #25.04, and #25.06 files were used up to the full WL. Group 3: Twisted File™ Rotary System. The canals were instrumented at a rotational speed of 300 rpm as follows: (a) #25.08 file was used up to the coronal one third of the root canal, (b) #25.06 file was used up to 4 mm short of the WL, and (c) #25.04 and #25.06 files were used up to the full WL. After the use of each file, the root canals were irrigated with 3 mL of a freshly prepared 1% sodium hypochlorite solution (Roval, Recife, Brazil). Glyde™ (Dentsply/ Maillefer) was used as a lubricant during instrumentation. A single operator experienced in rotary systems prepared all root canals. Each instrument was changed after five canals. Instruments were examined after every use to record and reject deformed or fractured instruments. Obtaining the postoperative images After instrumentation with files F1 and F2 (group 1), #25.04 and #25.06 (group 2), and #25.04 and #25.06 (group 3), the specimens were removed from the molds and the apical third section was viewed again in the stereoscopic magnifier with ×10´ magnification, the postoperative images being captured by a computer. Evaluation of centering ability Using the Image Tool software (University of Texas Health Science Center, San Antonio, TX, USA), the preoperative and postoperative images were compared (Figure 1). According to a previously described method19 , the following equation was devised to evaluate centering capacity (Figure 2): D1: X1/ X2 = (X1 “ X2 1)/(X2 “ X2 2) D2: Y1/ Y2 = (Y1 “ Y2 1)/(Y2 “ Y2 2) Where D1= the buccolingual measurement and D2 = the mesiodistal measurement. According to this equation, a result of 1 indicates perfect centering. Statistical analysis of the data The data regarding D1 and D2 were calculated from the usual location measurements (mean and average) and dispersion (standard deviation, minimum and maximum) at the 95% confidence interval. The results were statistically analyzed using the Student’s t-test and the Mann-Whitney test (statistical inference). A level of significance of 0.05 was adopted, using the Statistical Package for the Social Sciences, version 13 (SPSS Inc., Chicago, IL, USA). Results Table 1 presents the main descriptive statistics of the buccolingual measurement (D1) and mesiodistal measurement (D2) according to the diameter of the instrument used and the group to which the instruments (ProTaper Universal™, ProFile™, or Twisted File™ Rotary Systems) belong. This table shows that the means of D1 ranged from 0.79 to 1.5. The largest deviation was registered to instrument #25.06 in group 2. The means of D2 ranged from 0.86 to 1.52, with the largest deviation being registered to instrument #25.04 in group 3; however, there were no statistically significant differences (p>0.05) among the three groups nor among the instruments in the same group in terms of centering ability. Discussion Root canal shaping comprises one of the fundamental stages of endodontic treatment2. However, the presence of curvatures may pose difficulty in root canal instrumentation. The results of shaping curved root canals is influenced by several factors, such as flexibility and diameter of the endodontic instruments, instrumentation techniques, location of the foramen, and hardness of the dentin. Ledge formation, blockages, perforations, and apical transportation are undesirable accidents that have occurred during preparation of curved root canals20 . The introduction of NiTi instruments allowed a safer and easier preparation of canals with complex anatomic characteristics21. Several NiTi rotary instrument systems have been introduced to endodontics9. These instruments offer greater flexibility and more resistance to torsional separation than stainless steel files17. Because of these features, they are better able to maintain curvature even in severely curved canals. By preserving the original canal as far as possible, iatrogenic complications arising from cleaning and shaping can be avoided22. To reduce canal aberrations, new NiTi instruments have been developed, such as the systems investigated in this study. An increasing number of NiTi rotary systems have been marketed by various manufacturers. The choice of the instruments used for this study took into account several factors that make them different from other systems, such as cutting blades, body taper, and configuration of the file tip. The ProFile™ rotary system has been available for some years, having become a system with which other NiTi enginefiles are compared. The same manufacturer has introduced another instrument of different design, the ProTaper™ system, purportedly to enhance cutting efficiency and improve flexibility of the instrument23. The ProTaper™ NiTi rotary system has been upgraded to the ProTaper Universal™ system, which differs essentially in the cutting blade designed for increased flexibility, cutting, and efficiency with a low proportion of apical deviation as demonstrated in the present and previous studies1,12-14. Ünal et al.24 has evaluated whether changes in the ProTaper™ system contributed to their shaping ability in terms of the morphology of curved canals. The authors observed that the ProTaper™ modifications did not create any discrepancy in the shaping abilities of the instruments. These findings are in contrast to previous studies25-27 in which the ProTaper Universal™ showed a greater tendency to produce apical transportation. A number of methods for investigating the effectiveness of endodontic instruments in shaping root canals have been used1,3-6,8-9,11-12,19,22-25. One of these is the use of the radiographic platform22,28-29. It merely provides, however, a two-dimensional image, precluding observation of the three-dimensional conformation of root canals. In the present research, as with previous studies3,30-31, the preoperative and postoperative images of the sectioned root canals were viewed by using a stereoscopic magnifier with ×10´ magnification and were compared using the Image Tool software, in which the centering ability of the NiTi rotary systems was assessed. This method allows a relatively easy and repeatable comparison of pre- and postinstrumented canals so as to analyze the action of the instruments on the root canal walls32 . Another method of analysis is computed tomography, a noninvasive method for analyzing canal geometry and the efficiency of shaping techniques5,10,26,33-34. With this technique, it is possible to compare the anatomic internal structure of the canal before and after instrumentation, but it was not used in this study. Human teeth were used in the present study, as in previous ones1,3,5,9,11-12,22,28,31,33-34. The main reason for choosing human teeth is that they simulate clinical conditions better than do acrylic blocks. Acrylic resin is not an excellent material for testing rotary instruments because it does not reproduce the microhardness of dentin and the frequently encountered anatomic variations (enlargements, oval root canals, etc), which cannot be easily simulated35. Mesiobuccal root canals of extracted human mandibular molars were used herein because they usually present an accentuated curvature36 . Several studies have used the Schneider method37 to determine root canal curvature5,11,22,33,36. In the present study, curvature was measured by the CAA method because it is as effective as the Schneider angle in evaluating root canal curvature and is better to measure the centering ability of root canal instruments18 . Although the ProTaper Universal™ rotary system supplies instruments with larger apical diameters, this study was limited to the F1 and F2 instruments in order to standardize the final apical preparation diameter to size 25 for the three groups. We showed that the three different rotary systems with distinct designs produced similar results in terms of centering ability. Analysis of the D1 measurement, in the present research revealed the largest deviation to be registered to instrument #25.06 of the ProFile™ rotary system when compared with the other systems; this is in agreement with the results demonstrated by Vanni et al.38. Nevertheless, Al-Sudani and Al-Shahrani11 demonstrated that ProFile™ produced centered preparations. This distinct performance could be attributed to the different designs of this instrument. ProFile™ instruments use a U-shaped file design with radial land areas, and have a neutral or slightly negative rake angle. Ersev et al.8 have shown ProFile™ to be significantly superior to other systems in terms of centering ability and Yamashita et al.39 reported that ProFile™ had the best cleaning ability compared with Quantec and Pow-R systems. In the D2 measurement, the highest value of deviation was registered to instrument #25.04 of the Twisted File™ rotary system. Gergi et al. 5 were the first to compare the centering ability of Twisted File™, Pathfile-ProTaper™ and conventional stainless steel K-files. They observed that the best centering was achieved with the Twisted File™ rotary instruments. El Batouty et al.40 reported that Twisted File™ produced significantly less transportation and preserved the original canal to a greater degree than did the K3 system. Although none of the instruments evaluated in this study was totally effective in performing biomechanical preparation of the root canals, because each of them produced morphological changes, the ProTaper Universal™, ProFile™, and Twisted File™ Rotary Systems demonstrated an acceptable capacity to shape curved root canals. There were no significant differences among the three groups or among the instruments in the same group in terms of the centering ability. Considering the limitations of this study and the fact that the Twisted File™ is new to the arsenal of endodontic tools, further investigations are required to provide more information about this new rotary system. Although none of the instruments evaluated in this study was totally effective in performing biomechanical preparation of the root canals, because each of them produced some morphological changes, ProTaper Universal™, ProFile™, and Twisted File™ Rotary Systems demonstrated an acceptable capacity to shape curved root canals. References
Copyright © 2011 - Brazilian Journal of Oral Sciences The following images related to this document are available:Photo images[os11058f1.jpg] [os11058t1.jpg] [os11058f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}