 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Prevalence of oral mucosal lesions and variations in Indian public school children Ambika L.1, Vaishali Keluskar 2, Shivayogi Hugar3, Sudha Patil3
1Department of Oral Medicine and Radiology, School of Dental Sciences, Krishna Institute of Medical Sciences University, Karad, Maharashtra, India, 2Department of Oral Medicine and Radiology, KLE VK Institute of Dental Sciences, Belgaum Karnataka, India 3Department of Pediatric Dentistry , KLE VK Institute of Dental Sciences, Belgaum Karnataka, India Received: August 28, 2011 Code Number: os11059 Abstract
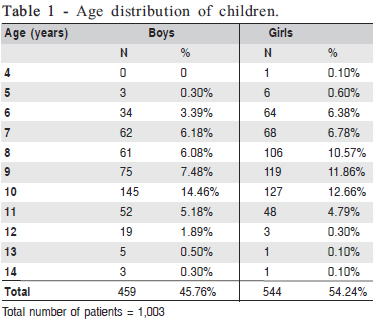
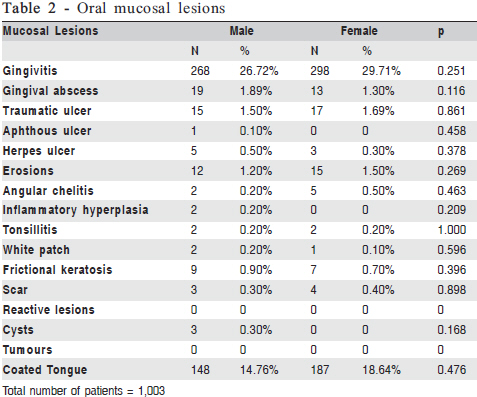
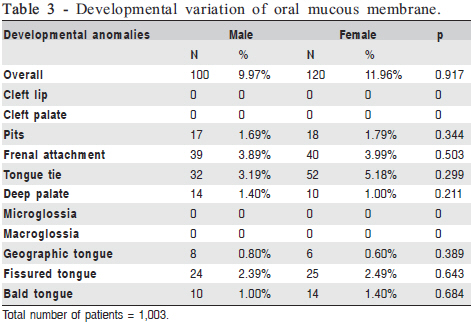
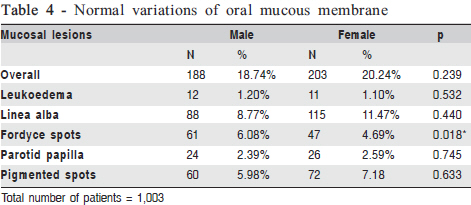
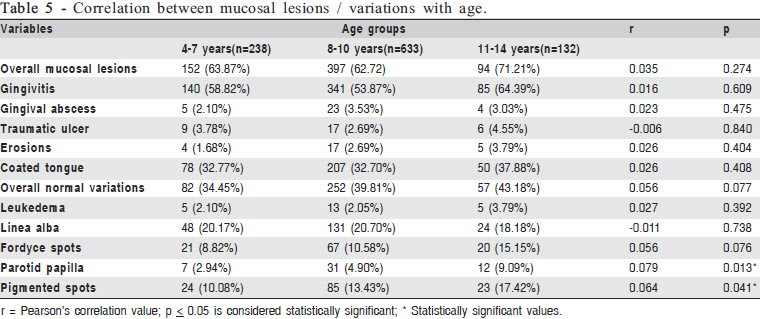
Aim: To study the nature and distribution of oral mucosal lesions and variations in children. Keywords: children, oral mucosal lesions, oral mucosal variations, developmental mucosal variations. Introduction The oral cavity is considered as a mirror of general health. The tongue lesions fissured tongue, geographic tongue, median rhomboid glossitis and oral mucosal lesions Fordyce’s spots and leukedema are classically considered as developmental lesions and normal conditions rather than having virtual disease characteristics. These lesions may be present at birth or become evident later in life1. Mucosal lesions may be discovered during routine dental examinations and vary depending on age, gender and /or race. Majority of oral diseases are confined to oral tissues, but numerous underlying systemic conditions may manifest with signs and symptoms within the oral cavity2 . Shulman3 (2005) studied 10,030 individuals aged between 2 and 17 years, out of which 914 individuals had 976 lesions. The lip was the most frequent site of lesions (30.70%), followed by the dorsum of the tongue (14.70%) and the buccal mucosa (13.60%). Lesions were more prevalent in males (11.76%) than females (8.67%). The most prevalent lesions were lip/cheek bite (1.89%), followed by aphthous stomatitis (1.64%), recurrent herpes labialis (1.42%) and geographic tongue (1.05%). In a study involving Turkish children, found that excessive melanin pigmentation (6.9%) was the most common lesion in the study population4. A crosssectional survey on 1,211 Brazilian children by Bessa, et al.5 (2004) found mucosal lesions in 27.0% children. The most common lesions were geographic tongue, cheek biting, and melanotic macula. They also concluded that the frequency of mucosal alterations in children was high and increased with age, and some of them were associated with habits and systemic problems. A study in Spanish children revealed that 30.92% children had oral mucosal lesions6 . Studies on oral mucosal lesions in Indian subcontinent are limited. A single study from India by Mathew, et al.7 (2008) studied prevalence of oral mucosal lesions in patient aged 2-80 years. Out of 243 children/adolescent only 41(16.87%) had mucosal lesions. In his study the sample size was too small to generalize the results. The present study was undertaken to highlight the nature of oral mucosal alterations and lesions among 4-14-year-old children and to study the influence of age and gender on oral mucosal lesions. Material and methods The study sample consisted of 1,003 children aged 4 to 14 years. Ethical clearance was obtained from the Institutional Ethics Committee to examine these children and also permission was obtained from the parents and teachers who were accompanying the children. Initially all primary schools children underwent regular screening after which children with oral problems were referred to the Department of Pediatric Dentistry for further dental examination and treatment. Children were informed briefly about the procedure involved. Children without parent’s and teacher’s consent were excluded from the study. Children suffering from any chronic illness were also excluded from the study. The examination was performed by one qualified and two trained dentists using plain mouth mirror under adequate illumination. Children’s detailed history was noted. Mucosal lesions, normal mucosal variations and developmental abnormalities were recorded in the specially designed proforma. A minimum of 10 children were examined per day over a period of 6 months. The data were compiled and analyzed using Statistical Package for Social Sciences software (SPSS Inc., Chicago, IL, USA) version 14. Descriptive statistics, chi-square test and Pearson’s correlation tests were used for analysis. For tests of significance p value d” 0.05 was considered as significant. Results There were 459 (45.76%) boys and 544 (54.24%) girls. Most of the children were in the age group of 6-12 years. Only few children were aged 4,5,13 and 14 years old (Table 1). As much as 643 (64.11%) children had mucosal lesions. Gingivitis was most commonly observed in 268 (26.72%) boys and 298 (29.71%) girls. Traumatic ulcer was observed in 15 (1.5%) boys and 17 (1.69%) girls. The most common sites for traumatic ulcers were the buccal mucosa (n=12), lower lip (n=10), upper lip (n=6) and tongue (n=4). The third most common mucosal lesion observed were superficial erosions of the oral mucosa. They were observed in 12 (1.2%) boys and 15 (1.5%) girls and the most common site for occurrence of erosion was the buccal mucosa (n=16), upper lip (n=6), lower lip, palate (n=2) and floor of the mouth (n=1). Children were also screened for reactive lesions, but they were not evident among them. Mucosal lesions were common in both the sexes with no statistically significant difference. Most children, 148(14.78%) boys and 187(18.69%) girls, had uncleaned tongue and associated halitosis. The other mucosal lesions observed are depicted in Table 2. Developmental oral mucosal variations were observed in 100 (9.97%) boys and 120 (11.96%) girls. High frenal attachment was observed in 39 (3.89%) boys and 40 (3.99%) girls. Ankyloglossia was observed in 32 (3.19%) boys and 52 (5.18%) girls. Among these, 80 had partial ankyloglossia and 4 had complete ankyloglossia. Fissured tongue was observed in 24 (2.39%) boys and 25 (2.49%) girls. Other developmental disturbances of oral mucosa are shown in Table 3. Microglossia, macroglossia, cleft lip and palate were not evident among any subjects. Normal oral mucosal variations were also studied. As much as 188 (18.74%) boys and 203 (20.24%) girls had these variations. Linea alba buccalis was present in 88 (8.77%) boys and 115(11.47%) girls. Fordyce’s spots were present in 61 (6.08%) boys and 47 (4.69%) girls. Among all the mucosal lesions/variations, only Fordyce’s spots were significantly (p=0.018) common in boys than girls. For rest of the lesions, there were no gender differences. Other developmental variations are represented in Table 4. Data were analyzed to find out any correlation between commonly occurring mucosal lesions/variations with age. Developmental variations were not included in the analysis because they are likely to be present since birth and unlikely to change as the age advances. The findings are described in Table 5. Among the studied variables, only parotid papilla (p=0.013) and pigmented spots (p=0.013) had significant positive correlation with age. Discussion Prevalence in earlier studies varies from 4.1 to 52.6%8 . In this study, children refered to the Department of Pediatric Dentistry were examined and 643 (64.11%) had mucosal lesions. As a routine, children are screened for any dental problems and those who require further treatment are sent to the Department of Pediatric Dentistry. The developmental variations of mucosa were evident in 220 (21.93%) children and normal oral mucosal variations were present in 391 (38.98%) children. Distribution of mucosal lesions/variations were same among both genders except for Fordyce’s spots (p=0.018). Parotid papillae and pigmented spots had significant positive relation with age and the rest of the lesions did not vary with age. Each type of mucosal lesion is discussed below. 1. Mucosal lesions Gingival Diseases In the present study, gingivitis was seen in 268 (26.72%) boys and 298 (29.71%) girls, thus comprising 56.43% of total population. Frequency of gingivitis was difficult to determine because of the lack of agreement on measurement criteria. Many studies have concluded that gingivitis begins in early childhood and that 9-17% of children aged 3-11 years present with gingivitis. At puberty, prevalence rises to 70-90%9. In the present study, only 3.2% children had gingival abscess. Gingival abscess (dental abscess) is an acute lesion characterized by localization of pus in the structures that surround the teeth10 . Traumatic ulcers Traumatic ulcer was seen in 32 (3.19%) children and the most frequent sites affected were buccal mucosa in 12 (1.2%) followed by lower lip in 6 (1.0%). Traumatic ulcerations are considered to be the most common oral ulceration. In a study by Shulman3 (2005), most prevalent lesions were lip/cheek bite (1·89%). These ulcers may be caused by direct physical/ mechanical, thermal or chemical trauma to the vascular compromise, causing tissue damage and ulceration11. Aphthous ulcer was seen in 1 (0.1%) child with a history of recurrence once in 6 months. Superficial erosions of oral mucous membrane were observed in 2.7% children. Sites affected were buccal mucosa 16 (1.6%), upper lip (0.6%), lower lip and palate (0.4%) and floor of the mouth 1 (0.1%). All causes were due to trauma from toothbrush, hot food and dental instruments. Herpes simplex infection In the present study, children with lower socioeconomic status had herpetic ulcers. Among 8 (0.8%) children, 6 (0.6%) had vesicles and ulcers on the upper lip, 2 (0.2%) had ulcers on lower lip and palate respectively. A previous study reported prevalence of 0.78-5.2%8. All children gave a positive history of prodromal symptoms. Most cases of primary HSV-1 infections are subclinical and generally occur in children and teenagers. There is a 1-to 3-day viral prodrome of fever, loss of appetite, malaise and myalgia that may also be accompanied by headache and nausea11 . Angular cheilitis In the present study, 7 (0.7%) children had angular cheilitis and all had pallor on general physical examination. A study on Turkish children reveled that angular cheilitis was the only oral mucosal lesion that had a significant correlation with anemia12. Angular cheilitis is infected fissure of the commissures of the mouth, often surrounded by erythema. The lesions are frequently coinfected with both candida and staphylococcus aureus. Other factors like vitamin B12 deficiency and iron deficiency have been associated with this disorder. Atopy has also been associated with the formation of angular cheilitis13 . White lesions In the present study, 3(0.3%) children had homogenous, thick, non-scrapable, white patch on the buccal mucosa suggestive of oral leukoplakia. All children had a habit of chewing gutka (a chewing preparation using areca nut and tobacco) since 2-3 years. History revealed that gutka chewing habit was learnt from their parents. Frictional keratosis of buccal mucosa due to of sharp teeth was observed in 16 (1.6%) children. Frictional keratosis is defined as a white plaque with a rough and frayed surface that is clearly related to an identifiable source of mechanical irritation and that usually resolve on elimination of irritants. Lesions belonging to this category of keratosis include linea alba and cheek, lip and tongue chewing. It is frequently associated with sharp cusps and edges of broken teeth14. Leukedema In the present study, 12 (1.2%) boys and 11(1.1%) girls had leukoedema. The total prevalence was 2.2%. Leukoedema was alleged to occur only in adult population until Martin and Crump15 found this lesion in children and in youths. Leukoedema is a common mucosal alteration that represents a variation of the normal condition rather than a true pathologic change. It has been reported in up to 90% of black adults and up to 50% of black teenagers. The most frequent site of leukoedema is the buccal mucosa bilaterally, and may be seen rarely on labial mucosa and soft palate14 . Linea alba buccalis In this study, 88(8.8%) boys and 115(11.47%) girls had linea alba buccalis. Total prevalence of this mucosal variation was 20.27%. It is a normal variation in the buccal mucosa that appears as a white line beginning at the corners of the mouth and extending posteriorly at the level of the occlusal plane. It is a very common finding and it is most likely associated with pressure, frictional keratosis, or suction trauma from the facial surfaces of the teeth. It is usually present bilaterally and may be pronounced in some individuals. These white lines may disappear spontaneously in some people14 . Fordyce’s spots In the present study, 61 (6.08%) boys and 47 (4.69%) girls had fordyce’s spots and statistically significant difference (p=0.018) was observed among both the gender. These tubuloacinar sebaceous glands found in the vermillion border of the lip, buccal mucosa and occasionally on the palate, gingiva and tongue. The number of Fordyce granules increases with age and is not correlated with systemic atherosclerosis and smoking. Men usually exhibit more Fordyce’s granules than women exhibit16. This finding was consistent with the present study. Oral pigmentations In the present study, 132 (13.16%) children had normal physiological pigmentation on the tongue and buccal mucosa. Oral pigmentations had significant positive correlation (p=0.041) with age. This may be true as some of the factors like smoking induced, hormone induced and drug related pigmentations are likely to increase as the age advances17.A study by Mumcu, et al.4 (2005) in Turkish children found that excessive melanin pigmentation (6.9%) was the most common oral mucosal lesion. Erica Amir, et al.17 (1991) conducted a study to investigate the prevalence of physiologic pigmentation in Israeli Jewish children of different ethnic origins. A total of 1,300 6-10-year-old children were examined. Physiological pigmentation was found in 13.5% of the population studied. Children of Eastern origin showed a significantly higher prevalence of pigmentation compared with Ashkenazi and Sephardic groups. Because melanin pigmentation can be enhanced by mechanical and chemical stimulation (smoking), this study may serve as a baseline for investigation of melanin pigmentation in various ethnic groups. The melanotic macula in the mouth is equivalent to a freckle or brown pigmented patch of the skin. In children it is most likely racial in origin, in which case it may be called racial pigmentation or physiological pigmentation, and no treatment is necessary. Maculae were seen in 10(1.0%) children. Petechiae were seen in 22(2.2%) children and all were traumatic in origin. Cysts and tumors In the present study, only 3(0.3%) children had mucoceles. The location of these mucoceles was lower lip, floor of the mouth and buccal mucosa. Tumors were not noticed in any subjects. Mucoceles, which are of minor salivary gland origin, are also referred to as mucus retention phenomenon and mucus escape reaction. Data from the Third National Health and Nutrition Examination Survey (NHANES III) that included 17,235 adults aged 17 years or older documented an overall prevalence ranking of 44 for the mucocele and a point prevalence of 0.02%. In the same study, which comprised of 10,030 children aged 2-17 years, mucocele had a point prevalence of 0.04%18. Oral vascular lesions, like hemangioma, vascular malformation and varix, are common19 but none was noted in our study sample. 2. Tongue lesions and anomalies Ankyloglossia (tongue-tie) In the present study, 84 (8.37%) children had tongue tie. Eighty (7.98%) had partial tongue tie and 4 (0.39%) had complete tongue-tie and children with complete tongue tie had speech problem. In previous studies, ankyloglossia was noted in 0.3%4 and 2.8%6. In our study, because of selective population, the number of children with ankyloglossia was high. Messner and Lalakea studied speech in children with ankyloglossia and noted that the phonemes likely to be affected due to ankyloglossia include sibilants and lingual sounds such as [t d z s θ ð n l]. Messner and Lalakea also examined speech and ankyloglossia in another study. They examined 15 patients and speech was grossly normal in all subjects. However, half of the subjects reported that they thought that their speech was more effortful than other peoples’ speech20 . In the present study, 79 (7.88%) patients had high frenal attachment and all had midline diastema seeking orthodontic consultation. Geographic tongue This is an annular lesion that affects the dorsum and margins of the tongue. The lesion is also known as erythema migrans. It is one of the most prevalent oral mucosal lesions, as prevalence may vary from 0.60-9.8%8. In this study, 14(1.4%) children had geographic tongue with no gender predilection and all were asymptomatic. The prevalence of this seems to decrease with age, which supports spontaneous regression over time11. In the present study, correlation with age was not analyzed as only few patients had geographic tongue. Complete bald tongue was seen in 10 (1.0%) boys and 14 (1.4%) girls. Nutritional deficiency was thought as one of the predisposing factor since these children did not have any other abnormalities. Fissured tongue In the present study, fissured tongue was noted in 49 (4.9%) children. There were 24 (2.39%) boys and 25 (2.49%) girls and all had shallow grooves. The prevalence of fissured tongue worldwide varies by geographic location and has been reported to vary from 1.49-23%8. Yarom, Cantony and Gorsky21 (2004) studied the prevalence of fissured tongue, geographic tongue and median rhomboid glossitis among Israeli adults of different ethnic origins and they found prevalence of FT was 30.5%. The most prevalent, typical fissured tongue, grooves over one third of the dorsal tongue, was noted in 11.5% of the study group. In the present study, when tongue was examined for cleanliness, 335 children had unclean tongue and associated halitosis. For all these children oral hygiene instructions were given after their examination. Congenital pits In the present study, 35 (3.5%) children had commissural lip pits and all had bilateral presentation. Gorsky, Buchner and Cohen22 (1985) studied the prevalence of commissural lip pits in a group of 2,462 Israeli Jews and found a relationship between commissural lip pits and ethnic background. Their results showed the presence of commissural lip pits in 17.4% and 9.7% were unilateral and 7.7% were bilaterally located. In this study, more than 50% of the children had mucosal lesions and variations. Only few oral mucosal lesions had gender differences and vary with age. Some of the lesions were symptomatic and some were not. Thus, this study helped revealing all unnoticed findings in children, which can facilitate the diagnosis of oral lesions at an initial stage. Routine oral examination is mandatory in children to identify lesions at an initial stage, thus facilitating their further management. References
Copyright © 2011 - Brazilian Journal of Oral Sciences The following images related to this document are available:Photo images[os11059t2.jpg] [os11059t5.jpg] [os11059t4.jpg] [os11059t1.jpg] [os11059t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}