 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Brazilian Journal of Oral Sciences, Vol. 10, No. 4, Oct-Dec., 2011, pp. 294-296 Using biomodels for maxillofacial surgeries: 10 years of experience in a Brazilian public service Gabriela Mayrink1, Luciana Asprino2, Roger William Fernandes Moreira2, Gustavo Henrique de Lima Paschoal3, Pedro Noritomi4, Márcio de Moraes2 , 1DDS, MsC, PhD student in Oral and Maxillofacial Surgery, Piracicaba Dental School, University of Campinas, Brazil, 2DDS, MsC, PhD, Associate professor in Oral and Maxillofacial Surgery Piracicaba Dental School, University of Campinas, Brazil, 3Eng., Renato Archer Center of Research, Product Development, Brazil, 4MsC, PhD, Renato Archer Center of Research, Product Development, Brazil Received: October 20, 2011 Code Number: 11060 Abstract
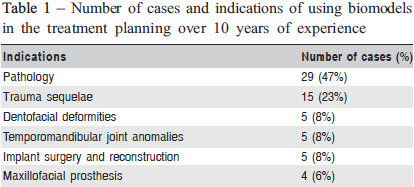
Aim: To evaluate 10 years of experience of use of biomodels at the Department of Oral and Maxillofacial Surgery of the Piracicaba Dental School, University of Campinas (UNICAMP), Brazil, showing the difficulties and importance of using biomodels in a public oral and maxillofacial surgery service. Keywords: technology assessment, biomedical, health planning, prototype. Introduction Biomodels have been used in treatment planning of oral and maxillofacial surgery since its introduction in 1985 by Brix and Lambrecht1-3. Currently, biomodels have been used in cases involving craniofacial deformities surgeries, extraoral implants, pathologies and trauma sequelae. The first and most common method to acquire biomodels is stereolithography. In this technique, the liquid resin is polymerized by laser light to form a solid material with the desired shape1. The model is created from many thin horizontal contour layers each 0.25 mm thick. These are fused on top of each other to form a 3D model4 . The other way to acquire biomodels is from selective laser sintering. This technique produces prototypes with fewer details, but it is less expensive. This article presents the outcome of the evaluation of 10 years of experience of use of biomodels in the Department of Oral and Maxillofacial Surgery of the Piracicaba Dental School, University of Campinas (UNICAMP), Brazil, showing the difficulties and importance of using biomodels in a public oral and maxillofacial surgery service. Material and methods The research protocol was approved by the Ethics Committee of Piracicaba Dental School/UNICAMP, Piracicaba, São Paulo, Brazil. Data were collected from the records of patients from the aforementioned Department of Oral and Maxillofacial Surgery, who were subjected to surgeries with use biomodels in the treatment planning, between January 2000 and December 2010. Computed tomography images that were used in fabrication of the biomodels were collected from the database of the Renato Archer Information of Technology Center -CTI, Campinas, Brazil. Results Biomodels were used in 63 cases. All biomodels used in these cases were made by the CTI. Table 1 summarizes the number of cases and indications of using biomodels in the treatment planning over 10 years of experience, which included mostly treatment planing of pathologies, trauma sequelae and others. Discussion The importance and advantages of using biomodels in the treatment planning are well defined in the literature. D’Urso et al. (1999)4, emphasized this advantages:
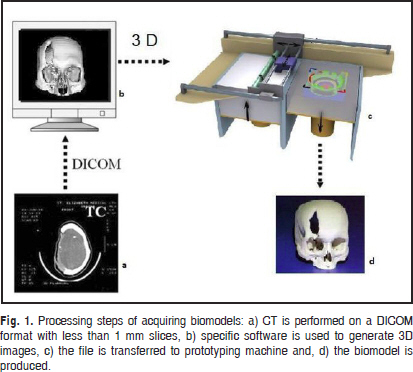
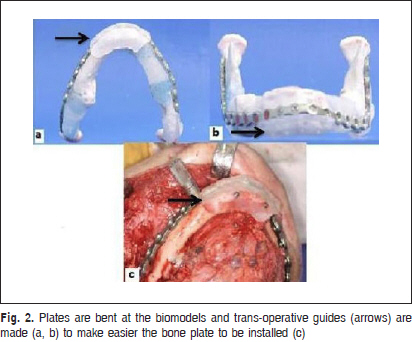
Erickson et al.5 emphasized that biomodels can take a mean time saving of 20% in expended operating room and anesthesia time. It could hypothetically minimize additional surgical trauma, blood loss, risk of infection and postoperative complications. Different methods can be used to make biomodels. The stereolithography apparatus machine starts with a tank of liquid resin and constructs from bottom to up. A laser beam selectively polymerizes ultraviolet sensitive liquid monomer on a platform suspended in a vat of the liquid and the platform is lowered by increments of 0.25 mm as each slice is polymerized. A multi-layered model is then built up as the contour slices are progressively fused together1. The main advantage of this technique is that the ensuing models can incorporate complete internal structure within a closed skull including sinuses and even intrabony neurovascular canals1 . However, stereolithography is a highly expensive method to manufacture biomodels. D’Urso et al.6 showed that the cost of the stereolithography in Australia is around U$1,000 per case. In Brazil, to manufacture a biomodel on a private service, the cost of the stereolithography (case complete: skull base, maxilla and mandible) is around U$3,200. This could preclude its use in a public service in Brazil. The Department of Oral and Maxillofacial Surgery of Piracicaba Dental School at the University of Campinas, in a partnership with CTI, enables the use of prototypes for treatment planning of patients of a public system of health using a less expensive method: selective laser sintering. Similar to stereolithography, original CT data are stored in a CD-ROM on a DICOM format. It is important to obtain images with 1.0 mm reconstructed slice not to lose details at the time of the confection of the biomodels. These data are transferred to the CTI for 3D image and laser sintering biomodel. The software Invesalius, created by CTI, is used to generate 3D images, compensate for dental restoration artifacts and monitor the effect of threshold values for segmentation purposes7. Then, the DICOM file is converted into STL format and this data is transferred to the selective laser sintering rapid prototyping machine to produce the biomodel. In our cases, the models of the patients are reproduced in cast resin through technology of 3D Printer Zcorp Machine (ZP 510, Zcorporation, Burlington, MA, USA), where layers of 1.0 mm in the axis Z are added together by a head printout with accuracy of 4.0 mm in X and Y axes (Figure 1) The high precision is important to decrease the chances of errors in planning. For example, in surgeries of trauma sequelae and pathologies, the osteotomies are performed in the biomodel and the trans-operative guides are made according to this model surgery to make easier the bone plate install (Figure 2). However, the occlusal splints are made in the normal sequence in the casts and the biomodel is useless to this stage. If the prototype is imprecise, the guide will make the bone remain poorly repositioned. Accordingly to this, Nizam et al.8 made a study to determine the dimensional accuracy of the skull models produced by rapid prototyping technology using stereolithography apparatus. They compared measures in the dry skull and their replicas and found that the percent difference was 0.08% with a standard deviation of 1.25%, concluding that biomodels are affordable to using in treatment planning in oral and maxillofacial surgery. In conclusion biomodels are an interesting tool in treatment planning in oral and maxillofacial surgery. In Brazil, the difficulties to obtain prototypes can be minimized by using selective laser sintering technique supported by the federal institute CTI. It is relevant to select cases in which biomodels are really important in the planning. At our public service, 63 patients have benefited from this technology without any costs to them and with good results, improving surgical planning and allowing the patients and their families figuring the perspective outcomes. References
Copyright © 2011 - Brazilian Journal of Oral Sciences The following images related to this document are available:Photo images[os11060f2.jpg] [os11060t1.jpg] [os11060f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}