 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Community Medicine & Primary Health Care, Vol. 16, No. 1, June 2004, pp. 4-9 Attitude of teachers to school based adolescent reproductive health interventions C. A. Iyaniwura Department of Community Health and Primary Health Care Olabisi Onabanjo University
Teaching Hospital, Sagamu. Code Number: pc04002
ABSTRACT
Adults may facilitate or obstruct healthy sexual behaviours by adolescents; hence information on their attitude towards adolescent sexual behaviour, including contraceptive use is important. The attitude of teachers to school-based adolescent reproductive health services was assessed among two hundred and twenty three teachers in Sagamu. Forty seven percent of them were trained family life educators while 52.9% had not received any training in adolescent reproductive health. Many of the teachers were aware of the common sexual and reproductive health problems of young people. Eighty seven percent approved of teaching sex education to adolescents in schools, 55.6% approved of contraceptive use by the adolescents and 52.9% approved of condom use. However, 52% of them believed contraceptive use should be initiated within marriage or after 18 years of age. Ninety-one percent of the teachers disapproved of condom demonstration and provision in schools. Only 36.2% were willing to counsel the sexually active adolescents about contraceptive use. Teachers indicated an interest in being involved in promoting the sexual health of their students but they preferred to counsel about abstinence. The family life educators had a more positive attitude to condom use than the other teachers; however this difference was not statistically significant. There is a need to educate teachers about adolescent contraception and why it is important for the sexually active adolescent to use contraceptives so as to protect their health and future, which the teachers also want to protect. KEY WORDS: Teachers, Attitudes, School-based, Adolescent, Sexuality Education
INTRODUCTION
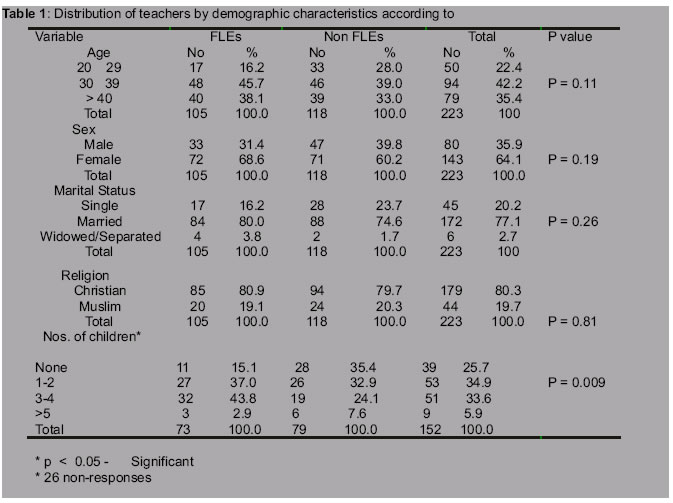
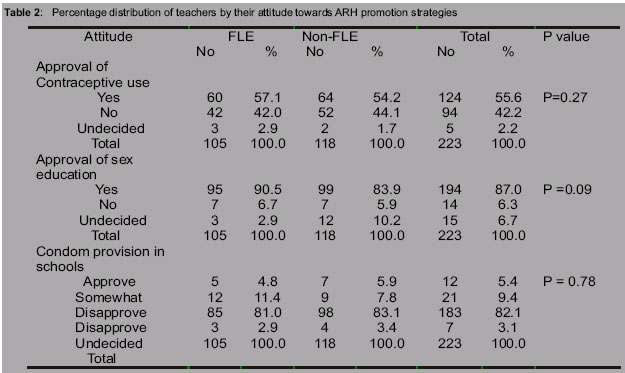
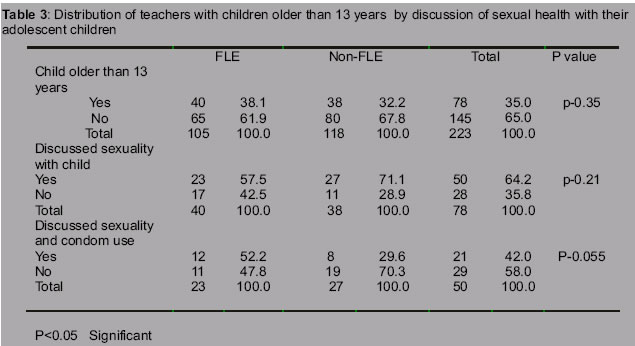
By the age of 20 years, majority of adolescents will be sexually active whether they are married or not. Among them, unprotected sexual intercourse with multiple or casual partners are rife. They do not use contraceptives and many of them lack the basic information about sexual matters and sexually transmitted diseases (STD). These result in a high rate of unwanted pregnancies and sexually transmitted infections (STIs), including HIV infection . Adolescents therefore need appropriate information and skills to help them take right sexual decisions. The school is one of the avenues to reach adolescents with reproductive health information especially in a country like Nigeria where primary school enrolment, especially in the southern part of the country is high (75% for girls and 86% for boys). This has the advantage of a captive audience with wide coverage. In the past few years many teachers in the Southwest of Nigeria have been trained to give sexual health information to adolescents. However, recent attempt to evaluate some sexuality education programmes revealed that resistance from teachers who were to implement the programme had limited the effectiveness of training2, 3. Evaluation has further suggested that giving health information may not be enough to encourage safe sex. Programmes must also teach adolescents how to use condom and make condom easily available in accessible places including schools to promote consistent and correct condom use4 . Presently, condom education and provision in schools has been introduced as part of AIDS control programme in some public schools in America5 . Unless programme implementers are convinced of the need for various strategies, interventions may not be effective. As important stakeholders in the school system, this study aims to assess the attitude of teachers to school-based adolescent reproductive health (ARH) interventions and suggest ways in which teachers' participation in ARH promotion can be improved. Each of the studied school had some teachers who have had special training in adolescent reproductive health (family life educators). It was assumed that family life educators (FLE) might have a more positive attitude towards ARH compared to other teachers who had no special training in ARH (non-FLEs). Hence the study compared the attitude of FLEs and non-FLEs. METHODOLOGYThis was a cross-sectional descriptive study conducted in the months of October and November, 2003. The target population was the teachers in public secondary schools in Sagamu, Ogun State in Southwest Nigeria. Seven secondary schools were selected among the nine public secondary schools in Sagamu through simple random sampling using balloting method. In the chosen schools, after consent was obtained from the principals or their representatives, the teachers were met as groups or as individuals and the objectives of the study were explained to them and their cooperation and consent sought for participation in the study. Structured questionnaires were administered to all the family life educators (FLEs) and all the other teachers who had no special training in adolescent reproductive health (non-FLEs) in each of the sampled schools. The questionnaires sought for information on the socio-demographic characteristics of the respondents, knowledge of common adolescent reproductive health problems, and attitude towards school-based ARH interventions and how they could be involved in promoting the sexual health of their students. A total of 225 questionnaires were administered to a total of 105 FLEs and 120 non-FLEs. The data was coded and computer analyzed using SPSS version 10. The results are presented in percentages and chi-square was used to determine statistical difference between groups. The level of statistical significance was p <0.05. RESULTS Of the 225 questionnaires administered, two were incompletely filled and were therefore discarded from the analysis. Table 1 summarizes the demographic data of the respondents. One hundred and five respondents (47.1%) were FLEs. A higher proportion of the non-FLEs were younger and single compared to the FLEs. Most of the respondents were married (71.9%) and were Christians (80%). Only 152 respondents (85.4%) of the respondents who were married or separated indicated the number of their children. Except for the number of children, there were no significant differences between the FLEs and non FLEs. To assess whether the teachers were aware of the common reproductive health problems of adolescents, they were asked to indicate whether they agreed or disagreed with certain statements. Eighty-six percent of the teachers agreed that sexual activity was common among youths, three-quarters agreed that sexually transmitted infections were common among them, only 67.6% believed that condom could protect against STIs and HIV. All the teachers were aware of at least one form of contraceptive method. Awareness of emergency contraceptive pill was low (19.4%). Table 2 summarizes the attitude of respondents to some ARH promotion strategies. Fifty-five percent (55.6%) of the respondents approved of contraceptive use by adolescents. The respondents were asked when an individual could start using contraceptives, 39.4% indicated that individuals should start after marriage, 39.4% believed an individual can start whenever the person starts having sex, 12.5% indicated after 18 years of age, while a minority believed it could be used by the age of 15 years (0.6%) and 13years (2.5%). A higher proportion (43.6% of the FLEs indicated that it should be used whenever an individual starts having sex compared to the non FLEs (35.4%). The difference was however not statistically significant (p > 0.5). Surprisingly, there were no significant differences between the FLE and non FLE in approval of contraceptive use, sexual activity and use of condoms among youths (Table 2). Condom was the most commonly approved contraceptive (52.9%). More FLEs approved of condom use by adolescents compared to non-FLEs (56.4% vs. 50%). Other methods that were approved of by minority groups included pills (8.5%), safe period (8.5%), and intrauterine contraceptive device (3.1%). Many of those who approved of contraceptive use by students however noted that premarital sexual activity is wrong; however, they recommended its use for the protection of youths from unwanted pregnancies and STIs. Eighty-seven percent (87%) of the respondents approved of the teaching of sex education in schools. Majority of them disapproved of the idea of providing condom in schools (90.5%) because they felt it could promote promiscuity, it is morally and religiously wrong and that a school is for education. Table 3 shows that 35% of the respondents had children older than 13years. Among those who had adolescent children, the non-FLEs were more likely to indicate having discussed sexuality issues with their children compared to FLEs (71.1% vs. 57.5%) but this was not statistically significant (p > 0.05). However, FLEs who had discussed about sexuality with their children were more likely to have discussed about condom use (56.5% vs. 29.6%). The teachers were asked whether they felt comfortable about discussing sexuality issues with youths, 70.6% indicated that they were comfortable doing so (71.8% of FLEs and 69.5% of non-FLEs). Sixty-nine percent had counseled adolescents about sexuality before (70.5% FLEs and 68.3% non-FLEs). To assess the aspect of ARH promotion strategies that teachers will most likely implement, they were asked how they could be involved in promoting the sexual and reproductive health of their students. Majority of the teachers were ready to counsel students about abstinence (83.8%). Only 36.2% were willing to advice them about condom use, FLEs (43.6%) were more likely to indicate so than non-FLEs (29.3%). Four point four percent (4.4%) were willing to teach about and provide condom for students. Fifty-one respondents (31.9%) were willing to refer sexually active adolescents to health workers when necessary.
DISCUSSIONS
Young people need correct information to help them make informed decisions about their sexual behaviour. When they are not given the appropriate information, they get half- truths and misconceptions from peers. Hence those who give young people sexual information must have adequate information, a positive attitude to ARH and must be ready to communicate such information to adolescents. In the study, the non-FLEs tended to be younger and single compared to the FLEs. Younger people and singles are more likely to have a less conservative attitude towards adolescent sexuality compared to older adults and the married 6; it was therefore not too surprising that the attitude of the non-FLEs to adolescent sexuality was comparable to that of the FLEs. Diffusion of information through interaction with FLEs and access to information about ARH through the mass media and printed materials may also account for the lack of significant differences in the two groups in attitude to adolescent sexuality. Forty-seven percent (47.1%) of the study population were FLEs. This is similar to the finding of a study in Nyanza, Kenya where it was found that less than half of the interviewed teachers had received any form of training in family life education 2. There is a need to train more teachers in adolescent reproductive health. Majority of the teachers (85%) agreed that there was a high level of sexual activity among students. Similarly, the result of participatory learning and action activities conducted among teachers and students in Oyo State of Nigeria ranked premarital sex among the first three major problems of the students 7. Many of the teachers agreed that sexually transmitted infections were common among youths (75%). However 32.5% of the teachers did not believe that condoms could protect against STIs and HIV. This may be as a result of the information that condom does not totally protect against HIV6. Such information may confuse the populace. Although abstinence is the best strategy for HIV control among unmarried youths, HIV education messages should continue to emphasize condom use as an effective means of protection in every risky sexual relationship. Forty two percent (42.2%) of the respondents disapproved of contraceptive use by adolescents. A comparable study of teachers at Port Harcourt, Nigeria found that 45.8% of them would not encourage girls to use contraceptives7 . Condom was the most widely known and most commonly approved contraceptive for adolescents. This may be due to the wide promotion of condom over the mass media. Many of the teachers did not approve of the use of other methods of contraception such as pills and injectables. There was a common misconception that the use of such methods can lead to future infertility. This misconception needs to be corrected. Fifty-two percent (52%) of the respondents believed that contraceptives should be used within marriage and after 18 years of age. This group of teachers may withhold contraceptive information from young adolescents. A study conducted among in-school adolescents in Ibadan (1995), showed that the average age at sexual debut was 13.8years 9. The first recorded case of HIV/AIDS in Nigeria was reported in a sexually active 13 year old girl. Therefore children must be given appropriate sexuality education even before they are sexually mature to help them make informed decisions. The teachers approved of sexuality education (87.5%) but the majority disapproved of providing condom in school. This attitude is reflected in how they felt they could be involved in promoting ARH. Four-fifths (79.8%) of the teachers were ready to counsel about abstinence and inform students about the consequences of premarital sex hence it is not surprising that 69% of the respondents had counselled adolescents about sexuality before. Thirty-six percent (36%) were ready to advice adolescents about condom use while only 4.4% were willing to demonstrate its use. Premarital sex is frowned at in this society; teachers feel that advising adolescents about condom use may suggest to young people that sexual activity is approved of among them. Religious inclinations of the teachers may also have a role to play in their reluctance because many of them indicated that premarit al sexual activity and providing contraceptives for adolescents is a sin. The findings of the study indicate that teachers are willing to promote the reproductive health of students but programmes that emphasize abstinence will receive better co-operation than those that promote safer sex. This is not surprising because evaluation of some school based ARH programmes have found out that some teachers refused to implement part of the sex education curriculum. In Peru, some teachers avoided teaching about AIDS and how young people could protect themselves2. This has implication for HIV control programmes. Although teaching about abstinence is good but for the sexually active adolescent, condom use can be life saving. Studies have shown that ARH programmes that focus on sexuality including sex, HIV education and safer sex did not increase sexual activity among youths 11, 12. Hence training of FLEs should examine the misgivings of individuals about safer sex promotion, emphasize the need for protection of the health of the sexually active adolescent and that programmes that teach about safer sex do not necessarily promote promiscuity. Only 31.9% of teachers were ready to refer students to health workers when necessary. If the school health programme is not well established or the health system works in parallel to the school-based programme, the teachers may not appreciate the importance of collaboration in promoting the health of adolescents. The attitude of teachers to referral can also be explained by the fact that teachers are not likely to hear about reproductive health problems of students unless consequences have occurred. Young people may be reluctant to discuss reproductive health problems with adults; they are more likely to patronize chemists, home made remedies or traditional healers12. Discomfort at discussing sexual issues with younger persons may limit communication about sexuality with adolescents. In this study, 30% of the respondents indicated that they were not comfortable with discussing sexuality issues with adolescents (even among FLEs) and it is not surprising that a similar proportion had never counseled adolescents about sexuality. These findings have implications for the adolescent school based reproductive health programmes. More teachers should be trained to help them appreciate the need to counsel adolescents not only about abstinence but also on why and how they can protect themselves when sexually active. Facts about the potential negative consequences of unwanted pregnancies and STIs must be emphasized. FLEs must be helped to examine their own biases in the light of scientific facts. Teachers must have factual information about adolescent contraception to debunk the myth that the use of contraceptives can lead to infertility. There is a need to identify those who feel uncomfortable about discussing sexuality issues with young ones, explore their misgivings, emphasize why they must communicate factual issues with young ones, desensitize their discomfort with sexual issues and allow enough time for practicing communicative skills during training. Emphasis should be placed on the fact that communicating information about sexuality does not necessarily encourage promiscuity or sanction it. Collaboration between health workers and the school system must be encouraged. Teachers should be informed of the reproductive health services that are available in the community. Refresher courses should be organized for FLEs periodically to discuss, practice communication with adolescent and update their information on adolescent reproductive health.
CONCLUSION
Teachers are aware of the common sexual and reproductive health problems of adolescents and they are willing to give them information to promote their health. However, they are more willing to encourage abstinence rather than contraceptive use. Majority of the teachers disapproved of condom demonstration and provision in schools. A higher proportion of family life educators approved of safer sex practices compared to other teachers but the difference was not statistically significant. There is room for improvement in the attitude of the teachers towards promotion of safer sex among adolescents, even among the FLEs.
ACKNOWLEDGEMENTS
The author is grateful to Prof. O.K Alausa of the department of Community Health and Primary Care, Olabisi Onabanjo University Teaching Hospital, Sagamu, for his useful comments. The co-operation and assistance of the teachers in the selected schools is highly appreciated.
REFERENCES
Copyright 2004 - Journal of Community Medicine & Primary Health Care The following images related to this document are available:Photo images[pc04002t1.jpg] [pc04002t3.jpg] [pc04002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}