 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Community Medicine & Primary Health Care, Vol. 16, No. 1, June 2004, pp. 10-15 Reasons and outcome of paediatric referrals from first-level health facilities in Sabongari, Zaria, Northwestern Nigeria. E. O. Musa and C. L. Ejembi Department of Community Medicine, Ahmadu Bello University, Zaria, Nigeria Code Number: pc04003 ABSTRACT Background: Referral is a crucial component of primary care
and when appropriately carried out is believed to result in favourable
outcome of illnesses. This study sought to determine the reasons and
outcomes of Paediatric (under-five) referrals from first-level health
facilities, and the factors influencing the outcomes. KEY WORDS: Child illness, Referral, First-level health facilities, Reasons, Outcome
INTRODUCTION
Nigeria's health policy which has identified primary health care as its fulcrum, defined a three tiered referral system for the management of patients.1 A network of primary health care centres in proximity to where people live, offering care of relatively low technology is the first level care from which patients gain entry into the health care system. Seriously ill patients beyond the management competence of primary health care workers are referred to secondary level general hospitals from where referrals are made to tertiary health facilities. The division of labour between the three complementary and easily recognisable levels seemed a rational, equitable and cost-effective way of dealing with the health care problems of the rural poor. 2 In consonance with this approach, the Integrated Management of Childhood Illness introduced in 1995 adopted this referral system for the management of children.3 First-level health facilities (health centres and out-patient services) in both rural and urban areas receive millions of sick children daily, most of them with one or more of the major causes of illness and death 3 Seven in every ten of the childhood deaths are due to five common, preventable or easily treatable conditions; namely, diarrhoea, pneumonia, measles, malaria and malnutrition, and often to a combination of these conditions. 4 These conditions account for over 70% of problems for which millions of parents or caregivers bring their children to a health facility or seek health care from pharmacists, community healthcare providers and traditional healers.5, 6. IMCI categorizes the sick children seen in these health facilities in two: Those with minor illnesses which can be treated at the facility or at home and those who are seriously ill and need care that usually cannot be given at that level. This latter category of survival chance. The proportion of referred children that actually get to the referral centers, access to such referral centres, the quality of care received and the outcome of care at the referral centres in Nigeria remain unknown. If strengthening the referral system is a crucial part of on-going health sector reforms and the effectiveness of IMCI then there is a need to study referral practices so as to provide evidence-based information for planning for provision of baseline data for evaluation of performance of the proposed IMCI interventions. This study is therefore aimed at determining the proportion of sick children referred from public PHC facilities who actually get to the referral centers and the quality and outcome of care received.
METHODOLOGY
Study area: The study was carried out in Sabon Gari Local Government Area (LGA) of Kaduna State in North-western Nigeria. It has a projected population of about 350,000. It is an urban LGA consisting of a cultural mix of various ethnic groups with Hausa as the predominant ethnic group. The local indigenes are predominantly farmers and traders while most of the settlers are public servants and students. There are many road networks in the LGA that connect the area with other towns within and outside Kaduna state, and they are mostly motorable all year round. The LGA owns a total of 22 PHC facilities consisting of eight family health units, nine health clinics and five health posts. These health facilities, all providing child health services, are distributed in six health districts. In addition, there are a total of 25 registered private clinics and hospitals and 12 institutional clinics belonging to either industries or training institutions. Numerous patent medicine vendors (PMV) and chemists and traditional medical practitioners also exist. The Ahmadu Bello University Teaching Hospital, located less than five kilometres from the centre of Sabon Gari LGA serves as the main referral centre for these health facilities. Study design: A cross-sectional descriptive study design was used to study a population of referred sick under-fives seen in public first level health facilities (HF) in Sabongari LGA. In each health district, one first level health facility was selected using simple random sampling by balloting. From September to December 2002 all the 106 referred sick under-five children seen in these sampled health facilities were recruited into the study. Four sets of data collection instruments were used by the researchers and six trained research assistants who were all primary health workers to collect the data. These consisted of: (i) structured, close-ended self-administered questionnaires for heads of the health facilities soliciting information on ownership of the facility, resource availability, service delivery, financing and referral policy; (ii) a two-way referral form with two sections (A&B) which was completed for each referred child by the referring health worker at the first level HF and the health worker at the referral centre respectively. Section A solicited for information on the presenting problems, diagnosis, treatment given, reasons for referral, place of referral and follow-up plans. Section B sought information on timeliness of arrival at the referral hospital, type of care received, duration of hospital stay and the outcome of care; (iii) a structured questionnaire which was used to conduct exit interview with the mother/caregiver of each of the referred children, and sought information on their satisfaction with the service received, the level of communication with the referring health worker, willingness to comply with the referral and residential address. In the very few cases where the researchers or the research assistants was not available at the HF at the time of the referral, the child and mother/care-giver were located at the referral hospital or at their residence to conduct the interview using the recorded address (iv) A management practice observational checklist which was used by the researchers or assistant to conduct a structured observation of the management practices of the referring health workers at the first level HFs and ascertain the quality of care and the authenticity of information provided by the health worker. It was not possible for the researcher and assistants to see all the referred cases at the very times they presented and exited. In cases where, consultations in the HF commenced before the notification of the researcher or assistant of the impending referral, information on management practice preceding the arrival of the researcher or assistant was collected retrospectively from the patient's case notes and the referring health worker. Data were computer analyzed using the SPSS statistical package. The analysis consisted of frequency distribution of the variables into tables and charts. Bivariate analysis using X2 test of statistical significance was used to determine the association between the variables.
RESULTS
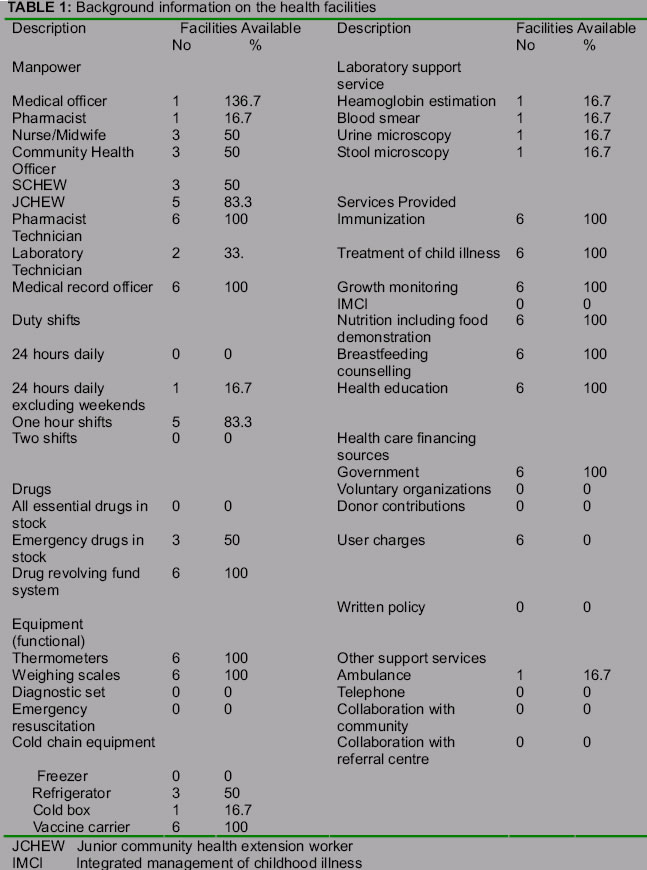
The background information on the health facilities (HFs) is outlined in Table 1. Only 3 of the 6 facilities met the minimum human resource requirement of at least one senior community health extension worker (SCHEW) per first-level PHC facility. One facility had a medical doctor; i.e., the Federal Government-owned (Army) facility, while three (50%) had either a nurse, community health officer (CHO) or SCHEW. Five of the six facilities had at least one junior community health extension worker (JCHEW). The predominant type of duty shift in the facilities was the one 8 hour shift, starting from 8:00 am, which was in operation in five of the six HFs. No HF had all essential drugs in stock while emergency drugs were available in only half of the facilities. However, all the facilities operated a drug revolving fund scheme. Equipment such as thermometer and weighing scale were available and functional in all the HFs but there were no emergency resuscitation equipment and diagnostic set in any of the facilities. The commonest cold chain equipment was vaccine carrier which was available in all the HFs. Three of the six facilities had functional refrigerators, none had a freezer and only one had a cold box. Only one facility possessed laboratory support services. All the facilities provided basic childhood services as listed in the table. All the HFs sourced their finances from government subventions and user charges. No HF had a written referral policy. Other referral support services were generally lacking in the facilities, for instance only one HF had an ambulance and none had telephone.
Reasons for referral
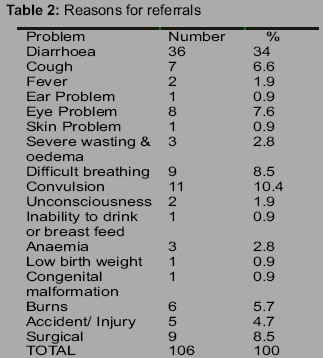
The reasons for referral for the 106 referred children are shown in Table 2, diarrhoea was the most common reason for referral (34%) followed by convulsion (10.4%), difficulty in breathing (8.5%) and surgery (8.5%). Other common reasons included eye problems (7.6%), cough (6.6%), burns (5.7%) and accidents/injury (4.7%).The most important reason given by the health workers for deciding to refer the children was for better diagnosis and treatment (70.8%) followed by severity of the condition (24.5%). Parent/caregiver's request accounted for 2.8%, and 1.9% were because the health worker felt the children would benefit from unorthodox care.
Compliance with referrals
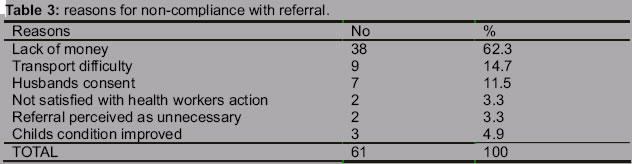
Of the 106 children referred, follow-up information was obtained for only 98 of the children. Majority did not comply with the referral as only 37.8% (37) of the 98 children were taking to the hospital. The most important reason for non-compliance was obtained from each of the 61 non-compliant referrals as outlined in Table 3. The commonest reason given was lack of money (62.3%) followed by transportation difficulties (14.7%) and denial of husband's consent (11.5%). The child's condition was said to have improved in 4.9% of cases and 3.3% were not satisfied with the health workers action or perceived the referral as unnecessary and so did not comply.
Outcome of referrals
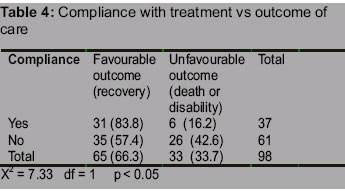
Fifty-seven percent of the non-compliant referrals had favourable outcome while 42.6% had unfavourable outcome. Of the 37.8% that complied, a greater proportion of them (83.8%) had favourable outcome (recovery) while 16.2% had unfavourable outcomes (death or disability). A statistically significant relationship was found between compliance with referral and the outcome of illness. (X2 = 7.33, df =1, P < 0.05)
Factors influencing referral outcomes
Twenty-seven (73%) of the children that arrived at the referral facility were managed as in-patients and ten (27%) as out-patients). All those that were managed as out-patients recovered, No referred child became disabled irrespective of the type of care received at the referral facility (i.e., in-patient or out-patient). Forty (65.6%) of the 61 non-compliant referrals received traditional medical care from traditional healers while 21 (34.4%) received various home-based remedies, with no outside consultations. The majority of those who had home management, 42.9% (17) recovered 33.3% (13) had one form of disability or the other, and 23.8% (10) died. A greater proportion of those who had traditional medication, 65% (14) recovered while 20% (4) had disabilities and 15% (3) died. There was no statistically significant association between the type of care received by the non compliant referrals and the outcome of care (X2 =2.67, df = 2, P > 0.05).
DISCUSSION
The study provides invaluable insight into the reasons and outcomes of the referral system for childhood illness in Sabon-Gari LGA, Kaduna State. The background information on the sampled health facilities revealed a general lack of resources (human and material) at the first-level health facilities (HFs) covered in the study. These findings are similar to the findings in several studies around Africa in which the same factors were found to militate against the referral process.8, 9, 10, 11. Effective case management requires appropriate access to drugs and consumables every day and adequately skilled health workers in the first-level facilities 12. Lack of communication, transport and poor organization of healthcare services adversely affect referral utilization and health outcomes. 13 This resource-poor health infrastructure situation is not helped by the fact that healthcare financing of the HFs rely mainly on government subventions and user charges which are not adequate in meeting the needs of the HFs. Community risk-sharing schemes such as a health insurance scheme can help reduce the economic burden of effective healthcare provision.10 Unfortunately no form of collaboration was found to exist between the HFs covered in the study and the community or the referral centers, in negation of the principles of primary health care. Community financing schemes for transport help alleviate transport difficulties. The commonest reason for referral was found to be due to diarrhoea (Table 2). Diarrhoea is a very common cause of morbidity and mortality in developing countries and is said to account directly and indirectly for between a quarter and a half of all sickness and deaths under the age of five years in the third world 3. This finding is in contrast to that of a study of paediatric referral in Tanzania in which anaemia and malaria were the main reasons for referral .13 It is also in contrast to a U.S study of family physicians' referral decision in which the commonest condition necessitating referral was surgical. 14 The finding in the Southern Tanzanian study is not unexpected particularly in an area with intense perennial malaria transmission, and low immunity among the under-fives. Anaemia may complicate malaria or result from a combination of factors such as poor nutrition and helminthic infection. Another reason for the Tanzanian difference may be because the HFs involved in the Tanzanian study perhaps had better laboratory services for the diagnosis of malaria and anaemia compared to the HFs involved in this study. The study found that the majority of the referrals (83.3%) that reached the referral centres recovered from their illnesses regardless of whether they received out-patient or in-patient care thus indicating that they received the type of care that was appropriate for their conditions at the referral centers. The total number of referrals that complied in this study is inadequate to apply the X2 test of statistical significance to determine the relationship between the types of care received at the referral hospital and the outcome of care. Generally, there is a dearth of information on studies of outcome of referrals in Africa. This study followed-up the referrals to determine the outcome of care at the referral facilities. Delay in arrival at the referral facility and the commencement of treatment at the referral hospital coupled with inadequate pre-referral treatment at the first-level facility may have contributed to the six deaths (16.2%) that were recorded. If providing emergency transport for emergency referral is impracticable in the majority of the HFs then invariably the role of time and monetary costs of transport would have also assumed great importance in determining the referral outcome. In many homes, seeking the husband's consent and financial constraints are other equally important factors that may delay or even hinder compliance to referrals. It is envisaged as evidenced in studies conducted in other developing countries, that the implementation of the IMCI strategy in all first-level facilities will help speed up the referral of the severely ill child and promote more favourable outcomes of illnesses. 15 The noncompliant referrals were also followed-up to determine the type of care received and the outcome of care The majority of the non-compliant referrals (65.6%) received traditional medication while 34.4% were managed at home using various home-based remedies. There was no statistically significant association between the type of care they received and the outcome. This perhaps, is because home management may involve self-medication and even herbal treatment which may not markedly differ from traditional medication hence the similarity in the outcome produced. Traditional medical practitioners are widely patronized in our communities even though they do not have a uniform system of operation. Some herbs have been found for instance to be useful in the treatment of febrile conditions. In consonance with the principles of primary health care, first-level health workers should be encouraged to collaborate with the traditional medical practitioners to identify such useful remedies. Linkages and collaboration must be encouraged between community health care providers, primary health care workers and health workers at referral centers if the problems of the referral system must be surmounted. This fact is particularly underscored by the fact that primary health care will not work without an efficient referral system supported by hospitals to provide continuity of care. Compliance with referral was found to affect illness outcome as a statistically significant proportion of the compliant patients had a more favourable outcome compared to the non compliant patients. This finding is consistent with the findings in many previous studies that referral of severely ill children lead to favourable outcomes. 3, 7, 16, 17. Referral is an essential part of preventing unnecessary deaths and health workers are expected to refer life-threatening illnesses which they are unable to treat properly. 13
CONCLUSION
The study found generally poor resource availability in the sampled health facilities as evidenced by lack of health personnel, inadequate supply of drugs, and lack of equipment, communication and transport logistics. The commonest reason for referral was diarrhoea closely followed by surgery. Majority of the health workers decided on referral for better diagnosis and treatment and due to the perceived severity of the condition. A greater proportion of compliant referrals resulted in favourable outcomes while a larger proportion of the non-compliant referrals had unfavourable outcomes such as death and disability. There is a need for adequate investment in resources at first-level health facilities to make referrals worthwhile and more effective.
REFERENCES
Copyright 2004 - Journal of Community Medicine & Primary Health Care The following images related to this document are available:Photo images[pc04003t2.jpg] [pc04003t4.jpg] [pc04003t3.jpg] [pc04003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}