 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Community Medicine & Primary Health Care, Vol. 16, No. 1, June 2004, pp. 25-28 Dental fluorosis and other enamel disorders in 12 year-old Nigerian children D.C. Umesi Koleoso Department
of Restorative Dentistry, College of Medicine, University of Lagos Code Number: pc04005 ABSTRACT Objectives: To determine the prevalence of dental fluorosis and other
enamel disorders in the study population, assess the degree of fluorosis, and
calculate the average number of teeth affected by different enamel disorders
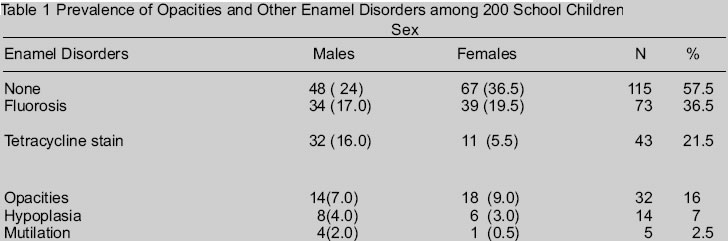
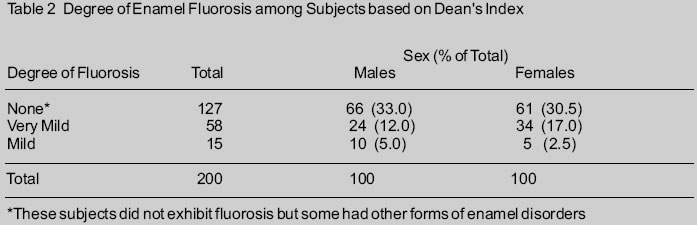
among 12year-old Nigerian children. KEY WORDS: Dental fluorosis, enamel disorders, 12 year-olds. INTRODUCTION Anomalies in enamel formation may either produce hypoplastic or hypomineralized enamel, this distinction sometimes being hard to sustain as some disturbances affect both matrix formation and mineralisation.1,2 The more commonly seen anomalies of enamel include dental fluorosis, tetracycline stains, enamel hypoplasia, enamel opacities, and enamel mutilation.3,4 Dental fluorosis occurs when individuals are exposed to high levels of fluoride (> 1 part per million) in water, food, toothpaste, salt and other media and especially when multiple sources of systemic fluoride are used in the same individual.5,6,7,8,9 Fluorotic defects are usually symmetrical and may present as faint white flecking of the enamel, paper white patches or striations or in severe cases yellow, black or brown staining of pitted enamel or hypoplasia of varying degree. In the very severe cases, the hypoplasia may lead to confluent pitting with associated loss of normal tooth form.3, 4, 5 The term “mottling” has also been used to describe the appearance of the enamel resulting from high fluoride intake during the period of tooth formation.10 Tetracycline staining of teeth occurs when tetracycline is administered to an individual during the tooth formative years.5 The teeth are at first bright yellow then become dirty brown or grey but show no structural defect of enamel.11 Enamel hypoplasia may manifest as minor structural defects of the teeth such as pitting or discolouration but occasionally, more serious hypoplastic defects are seen. These are usually indicators of past diseases or rarely of active disease.2,5 Enamel opacities that are idiopathic in nature may be seen in oral surveys.3 They are usually oval in form, non-translucent, not usually symmetrically distributed in the mouth and are seldom found on more than one or two teeth.12 A more specific kind of enamel opacity seen in oral surveys is that caused by dental fluorosis. Other enamel defects that are commonly seen are attrition and mutilation. The mutilations may sometimes be self-inflicted to create a midline diastema, which in some African cultures is regarded as a sign of beauty. Several studies have been carried out in different populations on the prevalence of enamel defects but comparisons have been difficult. This is because of the several classification systems that have been used for the various studies.13,14,15,16,17 It has been noted that the most suitable method of recording enamel disorders depends upon the aim of any particular study, for example whether one is considering the public health significance of enamel defects or assessing the detailed biological effects of fluoride.16 The indices may be broadly divided into two types; general or specific indices. The DDE index and the Jackson-Al-Alousi index are examples of general indices used to record non-specific hypoplasia, while the Dean Index, Tooth Surface Index of Fluorosis and Thylstrup Fejerskov Index are specific indices.3, 4, 12, 14, 16, 17 m This study is a pilot study involving 12year-old Nigerian children and it is aimed at recording the prevalence and severity of fluorosis and other enamel defects such as tetracycline stains, enamel hypoplasia, enamel opacities and enamel mutilation in the study population. Specific and non-specific indices were used in the study. Other studies involving children of this index age have been reported.18, 19 METHODOLOGY The study was done using the World Health Organization Pathfinder Methodology for Oral Health Survey.3,4 Children of age 12 years were selected from schools in the Lagos Mainland Local Government Area (LMLGA) of LagosState. Seven schools were selected from the list of schools obtained from the Local Government Education Department by simple random sampling. At the selected schools, 12 year-olds from the junior classes were randomly selected, ensuring that at each school at least 20 to 50 children and an equal number of boys and girls were seen. The subjects were examined seated on a straight back chair; daylight was the source of light. The teeth were examined in a wet state. Adequate sterile materials for examination were used and aseptic conditions observed. The Dean index criteria for fluorosis and the World Health Organization criteria for recording enamel disorders as outlined in its basic methods for oral health surveys was used for this study.3,4 The Dean’s Index criteria were used to record the degree of fluorosis.3,4 Other enamel disorders, such as tetracycline stain, opacities, hypoplasia, mutilation and attrition, were recorded if present. No attempt was made at aetiologic classification of the enamel hypoplasia in accordance with the research methodology.3,12 This is because children at the point of survey are usually unable to provide the history of infancy and childhood events required for such classification. The number of teeth affected by the enamel defects in each subject was recorded; from these the average number of teeth affected by each defect was calculated. RESULTS Of the 200 children examined, 57.5% had normal enamel while 36.5% had dental fluorosis of different degrees. Sixteen percent of the children had enamel opacities, 7.0% had enamel hypoplasia and 2.5% had mutilation of the anterior teeth caused by enamel fracture (Table 1). Attrition was not observed among the subjects. Based on Dean’s Index for fluorosis, 29.0% of the children had very mild fluorosis, while 7.5% had mild fluorosis (Table 2). The average number of teeth affected by the different enamel disorders among the sexes and the entire study population is presented in Table 3. The average number of teeth affected by enamel defects in the study population was 10.8 teeth for tetracycline stain, 6.3 teeth for enamel hypoplasia, 4.6 teeth for enamel opacities and 1.0 tooth for enamel mutilation. DISCUSSION Dental fluorosis was present in 36.5% of the subjects. With respect to the degree of fluorosis, 29.0% had very mild fluorosis while 7.5% had mild fluorosis based on Dean’s index.3,4 The level of fluorosis in the study population is less than that recorded by Nunn et al, who recorded 98% in children in Sri Lanka and 58% in children in England where the water fluoridation were 1.0ppm.15 Dental fluorosis occurs when the level of fluoride in drinking water exceeds the optimal level of 1ppm (one part per million). It may also occur when an individual is exposed to multiple sources of fluoride such as drinking water, fluoride containing toothpaste, salt, milk, fruit juices etc. When the prevalence of very mild and mild fluorosis is more than 22% it is likely that the community is being exposed to more than 1.5 ppm fluoride.5 It may then be necessary to reduce the level of fluoride they are being exposed to by defluoridating their drinking water. Young children often swallow toothpaste during toothbrushing, this may also account for the fluorosis recorded in this study as all the toothpastes manufactured in the country conform to the optimal level of fluoride. It may be necessary that local manufacturers of toothpaste introduce paediatric formulations into the market, which contain a much lower level of fluoride. Where the regular toothpaste is used, a peanut-sized strip should be applied to the toothbrush. Parents and caregivers need supervise young children during tooth brushing to prevent them consuming excess toothpaste. Discolouration of the teeth due to exposure to tetracyclines has been described since the introduction of this group of drugs in 1956.2 In this study 21.5% of the children had tetracycline stains. This figure is higher than those obtained by King and Wei, who recorded 16.9% in Chinese, 4.5% in Indian and 1.0% in White 12year-old children living in Hong Kong.13 Tetracycline is secreted in breast milk and it can cross the placenta to the foetus. Ingestion of tetracycline during infancy usually manifest in the permanent teeth. The administration of tetracyclines from 4 months to 6 years of age may cause severe clinical discolouration of permanent teeth.5 The degree of discolouration is affected by the particular type of tetracycline taken, the dosage, the duration of intake and the patient’s age at the time of administration. The more prolonged the course of treatment the broader the band of stain and the deeper the discolouration.11 Tetracycline stains are usually bilateral affecting teeth in both arches. As many as 8 to 20 teeth may be affected, depending on the duration of childhood exposure to the drug.5 The high prevalence of tetracycline stains seen in this study indicates that the drug is being given to the children either as home remedies by the mothers or on the prescription of the health personnel operating in these communities. Health education on the hazards of self-medication is needed in the communities, while the health profession needs to be re-sensitized to the dental implications of the administration of tetracyclines to nursing mothers and children below the age of 9 years. Fourteen subjects (7.0%) presented with enamel hypoplasia. This level of enamel hypoplasia is comparable to 3 15 % recorded in the general population.20 Hypoplastic defects may arise from local causes such as infections of deciduous teeth, which damage the underlying permanent successor. They may be due to systemic causes such as hereditary disorders, infections e.g. congenital syphilis and severe disturbances of metabolism arising from exanthematous fevers and other childhood infections.2,5 The enamel hypoplasia seen in this study may be associated with infections and exanthematous fevers of childhood. The level of tetracycline stains seen among the subjects is also suggestive of this. Enamel opacities were present in 16% of the children. This level of opacities is lower than the 33% in 12 14 year-olds reported by Soames and Southam.2 It is also lower than the 31% in 6 15 year-olds reported by Cutress and Suckling.21 This may be because these other studies involved a wider age range. These white patches may be due to local, systemic, genetic or environmental factors though the cause is largely unknown and they tend to get discoloured brown or yellow after tooth eruption as a result of deposition of oral pigments.2, 13, 22 Enamel mutilation was found in five children and these were due to incisal edge fractures. The low level of enamel mutilation observed in this study signifies a decline in the traditional practices of grinding or filing teeth to create midline diastema. Midline diastema is regarded as a sign of beauty in some cultures.3 The prevalence of a condition is usually determined by recording the “absence” or “presence” of that condition, however, it may be expedient to also determine the severity of the condition. When a condition is severe in addition to being prevalent, this calls for urgent intervention to ameliorate its effects and indeed take steps to prevent its further occurrence. The average number of teeth affected by tetracycline, opacities, hypoplasia and mutilation is used as a measure of severity of these conditions in this study, while the severity of fluorosis is measured by the degree recorded. Very mild fluorosis was recorded in 29.0% of the children, while 7.5% had mild fluorosis. The average of 10.8 teeth affected by tetracycline stains shows prolonged use of the drug in the subjects. Opacities are usually not symmetrically distributed in the mouth and are seldom found on more than one or two teeth.5 A higher number of teeth seem to be affected by opacities in this study with the average being 4.6 teeth. Hypoplastic enamel may be the result of disturbances affecting a single tooth, a group of teeth or all the teeth, thus, 1 to 32 teeth may be affected.2 In this study an average of 6.3 teeth is high and is indicative of disturbances affecting a group of teeth, such as occurs in chronologic enamel hypoplasia. Mutilation may involve one or both upper central incisors. An average of one tooth was affected by mutilation in this study. The role of ethnicity and socio-economic class was not examined due to the very small numbers recorded for some groups. Larger studies in future may address the effect of ethnicity and socio-economic class on enamel disorders. The World Health Organization form used for data collection did not provide for the recording of particular teeth affected by the enamel disorders. The form may be modified for future studies. This study of the prevalence of dental fluorosis and other enamel disorders in 12 year-old children in the Lagos Mainland LGA of Lagos State, showed that 36.5% had dental fluorosis, tetracycline stains was found in 21.5%, 16% had enamel opacities, 7.0% had enamel hypoplasia and 2.5% had enamel mutilation. In terms of severity, based on Dean’s index, very mild fluorosis was present in 29.0% while mild fluorosis was recorded in 7.5% of the subjects. The average number of teeth affected by tetracycline stains, opacities, hypoplasia and mutilation were 10.8 teeth, 4.6 teeth, 6.3 teeth and 1.0 tooth respectively. There is a need to intensify childhood immunization and health education efforts in the communities. This is with a view to reduce childhood diseases and the administration of tetracyclines in children below the age of nine years, thus, reduce the incidence of such enamel disorders as seen in this study. The different sources of fluorides, which may predispose the children to, multiple intakes of fluoride and hence dental fluorosis need to be identified. Nigerian- based toothpaste manufacturing companies may also consider the introduction of paediatric products, which contain a lower level of fluoride than the regular products. Parents should be more mindful of the amount of fluoride ingested by their infants and young children. The use of peanut-sized strips of the regular family toothpaste for children is recommended. It is also needful that government-run dental clinics and school oral healthcare programmes be established in the LGA to cater for the restorative treatment needs that arise from the high prevalence of enamel disorders in the communities. REFERENCES
Copyright 2004 - Journal of Community Medicine & Primary Health Care The following images related to this document are available:Photo images[pc04006t1.jpg] [pc04006t2.jpg] |
| |||||||||

{kind=link}
{kind=link}