 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Community Medicine & Primary Health Care, Vol. 16, No. 1, June 2004, pp. 29-32 Out-of-pocket health expenditure for under-five illnesses in a semi-urban community in Northern Nigeria. M. N. Sambo, C. L. Ejembi, Y. M. Adamu and A. A. Aliyu Department of Community Medicine, Ahmadu Bello University, Zaria, Nigeria Code Number: pc04007
ABSTRACT
Background: Household expenditure on health is increasingly becoming
a major source of health care financing in Nigeria. Recognizing the
limitations of this pattern of financing health care, the government
has introduced a social health insurance scheme policy that has provided
for government meeting the health care costs of children. However,
there is a dearth of information on the pattern and costs of under-five
illnesses at community level. This study therefore sought to determine
the magnitude and causes of illnesses among under-fives, sources of
healthcare and out of pocket expenditure among children under-five
in Layin Zomo, a semi-urban area of Northern Nigeria KEYWORDS: Healthcare, Out-of-pocket expenditure, Under-fives, Zaria
INTRODUCTION
Health care is a necessity and a basic human need. It is in recognition of this that the Alma Ata Declaration of the 1978 primary health care conference, endorsed by practically all governments, called for social guarantees that would ensure that the basic needs, including health and food of all people are met.1 Unfortunately, for most developing countries, the prospects of achieving even a minimal level of adequacy in health services and health remains a mirage. While health care needs is increasing, government expenditure on health in developing countries is declining.2The burden of disease which is greatest in Africa, is further worsened by the AIDS pandemic; conversely, Africa has the lowest health expenditure.2 Government expenditure on health in sub-Saharan Africa has severally been described as being inadequate, insufficient, inequitable and unsustainable2, 3 Rising poverty levels, increasing scale of health problems, the impact of economic policies, especially structural adjustment programmes have been identified as major contributory factors to the funding gaps between the health care needs and resources3, 4, 5. These have hindered geographical, financial and functional access to health care services.6The consequence of inadequate health expenditure which is more severe among the disadvantaged groups especially the women and children is further worsened by their disproportionately limited access to services thus additionally reducing the benefit of already scarce resources these groups most needs.7 In order to address the problems of poor financial access to health care, various options of health financing have been recommended. They include increasing household expenditure for health through inter- alia, user fees, social insurance and various forms of community finanacing.8, 9, 10 However, it has been documented that in most of the developing nations individual households already spent substantial amount of money in purchasing health care from the private sector, both modern and traditional.11 Notwithstanding the financing mix a country decides to adopt, it is imperative to give priority consideration to under-five children, given their importance as the future of any nation and their disproportionate vulnerability infectious diseases, poverty, malnutrition6 Nigeria, as a response to its health sector funding gaps has established a national social health insurance scheme.12 The country, in 2000 was adjudged to have the 15th worst under-five mortality rate out of 187 nations assessed6. In response to this, under the national health insurance scheme, there is a programme for under- five children for which government is “expected”to pay premium on their behalf for them to benefit from a defined basic health care package.13 The success of this programme will depend on evidence-based information that will assist policy makers in determining how much premium would be required to provide minimum health care package for the under-five children. This study was thus conducted with a view to determining the frequency and pattern of health problems, sources of health care as well as the current out-of-pocket expenditure on health care of under-five children in Layin Zomo, a semi-urban community in Zaria, Kaduna State, north-western Nigeria.
METHODOLOGY
The study was conducted in Layin Zomo, a peri-urban slum located in Sabon Gari Local Government Area of Kaduna State in north western Nigeria. It has an estimated population of 5,000 people made up of predominantly Hausa Moslems who are essentially subsistence farmers. The nearest public health facility to the settlement is a primary health care clinic located about 5 kilometres away, while the Ahmadu Bello Teaching Hospital is 10 kilometres away. However, there a few patent medicine stores in the settlement. The survey which was cross-sectional and descriptive in design was part of a community diagnosis undertaken within a four weeks period in the months of July and August 2004. Children aged 0 to 59 months constituted the study population from which a 50% sample of all such children in the settlement was drawn using systematic random sampling from household listing of all the households in the settlement. A total of 324 children were thus sampled for the study. In each of the selected households, information was collected on all eligible children from the mothers/caregivers. Structured, closed-ended, interviewer- administered questionnaires were used to collect information on type of health problems the children had in the three months preceding the study, where treatment was sought and the amounts paid for treatment. The total out-of-pocket expenditure for the treatment cost of treatment was computed and multiplied by four to get the total estimated cost for one year and this was divided by the total number of children studied to get the per capita out-of-pocket expenditure per child per year. The data which was collected by final year medical students were coded, and analysed using EPI info version 6 software package. Statistical methods used included frequency counts and tables.
RESULTS
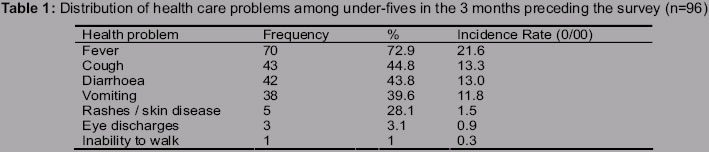
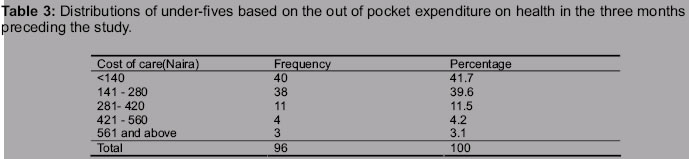
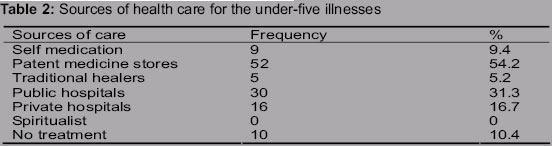
Of the 324 children 26.9% (96) were reported to have been ill in the three months preceding the survey. A proportion of the children had more than one bout of illness and many of them had multiple symptoms. The incidence rates of the reported health problems during the three months period were 21.6 per 1000 for fever, 13.3 per 1000 for cough, 13.0 per 1000 for diarrhoeal and 11.8 per 1000 for vomiting (Table 1). Of the 96 children that had been ill, fever was the leading complaint reported for 72.9% of the children followed by cough, 44.8% and diarrhoeal diseases, 43.8%. Other health problems reported during the period under review included vomiting (39.6%) and skin diseases (5.2%). Patent medicine stores were the source of treatment for majority (54.2%) of the illnesses. Public health facilities were used in 31.2% of the cases while 16.7% sought treatment from private clinics. Traditional healers were utilized in 5.2% of the instances while. 10.4 % do not seek for any form of treatment. Some of the respondents, 29.9% sought treatment from more than one source. The out of pocket expenditure for the treatment of each bout of illness treated ranged from less than 140 Naira (< $1) to more than 700 Naira (>$5). As shown in table 3 majority, 41.7% spent less 140 Naira (less than $ 1), 39.6% spent between 141 - 280 Naira ($1 -2), 11.5 % spent between 281 - 420 Naira ($2 - 3); only 3.1% spent 561 Naira and above ($ 5 and above). The median out of pocket expenditure on treatment was 171 Naira ($1.2). The estimated total out-of-pocket expenditure for one year was N82832 ($591.7), giving a per capita of 255 Naira ($1.8) for each under-five child.
DISCUSSION
The findings from this study revealed fever and cough; proxies of malaria and acute respiratory tract infections in children and diarrhoeal diseases to be the leading causes of illness among the study population. This finding is in conformity with the report on leading causes of illness among the study population. This finding is in conformity with the report on leading causes of morbidity and mortality among under-fives in Nigeria.14 Factors that determine pattern of utilization of health care services include geographical and economic accessibility, literacy level and perceived derivable benefits. The study found a higher patronage of patent medicine vendors compared to other sources of care with more than twice as many care givers utilizing their services for the care of the treatment of their under-fives compared to public health facilities. The high level of patronage of patent medicine vendors may not be unconnected with the absence of any public or private health facility within the community. The perennial lack of drugs in government owned health facilities and the low socioeconomic status of the study population may be added reasons for the preferential use of patent medicine vendors. Thus with meagre resources, under-five care givers can obtain treatment from nearby patent medicine vendors drugs no matter how inadequate the care may be. It is also important to underscore that most of the providers in the patent medicine stores lack any form of formal education that qualifies them to prescribe or dispense drugs. Unfortunately, in spite of their being major sources of health care provision, especially in rural areas where they may be the only sources of health care, there has been hardly any attempt by government to build their capacity for improved qualitative care provision. This is one area that the health sector reform agenda of the present the government of Nigeria and the national health insurance need to address in this country.15 It has long been established that general tax revenue which hitherto had been the main source of health care financing is no longer sufficient as a of health expenditure consequent upon the global economic recession, population explosion and inter-sectoral competing demands. 16 As at today, out-of-pocket expenditure represents about 43% of all expenditure in Africa, compared to 37% from government and about 25% from donors. However, while the per capita income in Nigeria is $260, the government expenditure on health is 14% while private expenditure is about 79.2%.17This shows that out-of-pocket expenditure is the main source of health care financing in Nigeria. The $5 per capita expenditure on health in Nigeria is far below the $14 recommended by World Bank for Africa18 and much lower than the $34 per capita recommended by WHO Macroeconomic Commission for Health for low income countries to provide basic health care services.19, 20 While information is not available on government's expenditure on health for the study population, one can infer that out-of- pocket expenditure is the major source of funding for childhood illnesses in the study community. The expenditure appears grossly inadequate as the annual per capita out-of- pocket expenditure per under-five child was $1.8. Given the comparatively low patronage of public health facilities by the residents of the study community for the treatment of their children's illnesses, this shows that their investment in the health of their children is very low. This may be a reflection of the level of poverty in the country as it is currently estimated that more than 70% are living below one dollar per day.21
CONCLUSION
This study has revealed the out-of- pocket expenditure for the treatment of under-fives in a poor peri-urban community. However, the values obtained may be grossly inadequate for giving direction in informing policy decisions on how much funds government need to provide under the national health insurance scheme for the provision of the proposed package of under-five care. This is because the amount of household out-of- pocket expenditure on health to a large extent is determined economic status. While others may explore out- of- pocket expenditure as a financing option given its merits in terms of mobilising resources, promoting efficiency, sustainability and private sector development, the pervading poverty in the land continue to pose a serious threat to its popularity especially among the poor. This underscore the need for more pro-poor policies like the proposed under-five social health insurance programme of the National Health Insurance Scheme. However, the success of this programme will depend on evidence-based information as well as adequate involvement of stakeholders in the conceptualisation and implementation of this programme.
REFERENCE
Copyright 2004 - Journal of Community Medicine & Primary Health Care The following images related to this document are available:Photo images[pc04007t3.jpg] [pc04007t1.jpg] [pc04007t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}