 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
SHORT COMMUNICATION Age at BCG administration during routine immunization. R.D. Wammanda , M.J. Gambo and I. Abdulkadir Department of Paediatrics, Ahmadu Bello University Teaching
Hospital, Zaria. Code Number: pc04008
SUMMARY
In Nigeria, as part of the National Programme on Immunization (NPI), BCG should be given at birth. A survey of the ages at which mothers bring their children for BCG vaccination showed that only 22% of children receive their BCG within the first 3 days of life and 36.2% within the first 7 days of life. The place of birth and whether a child was sick enough at birth to require hospital admission appears to be an important factor affecting the age at BCG administration KEY WORDS: Age at administration, BCG,
INTRODUCTION.
Bacille Calmette-Guerin (BCG) is the only available vaccine against tuberculosis1. BCG vaccination is the injection of a live attenuated strain of mycobacterium bovis to induce immunity to tuberculosis without exposing the vaccinated individual to the hazard of a natural infection2. BCG is best given at the age when individual passes from a time of low infection to one in which the chance of becoming infected is considerably high. In countries with low level of transmission, transition period is the adolescence, however, in the tropics, with high level of transmission, the changes occur at birth3. The official recommendation of the World Health Organization (WHO) is a single dose administered during infancy. This however varies from country to country. Studies have also shown that there is no significant difference in the mean tuberculin reaction, tuberculin positivity and the mean scar size in groups of children receiving 0.1ml of BCG at birth or at 4-6 weeks. 4 In Nigeria, as part of the National Programme on Immunization (NPI), BCG should be given at birth; at most within the first one week of life.5 In our Hospital, it has been observed that mothers bring their children at various ages for BCG vaccination. This study was therefore undertaking to determine the age at which mothers in our environment bring their children for the BCG vaccination.
METHODOLOGY
A structured questionnaire was administered on mothers who came to the immunization center of Ahmadu Bello University Teaching Hospital, (ABUTH) Zaria for routine immunization services. Consent for inclusion into the study was obtained from these mothers after explaining the nature of the study to them in the language they best understood. The questionnaire sought to know the age and sex of the child, age at BCG administration, gestational age at delivery, mode of delivery, place of delivery, whether the child was sick enough to require admission at birth and educational level of mothers. The birth weight was obtained from the child's card and the child examined for the presence of BCG scar. Test of significance was by the chi squared (X2) test where necessary. A P value of <0.05 was considered significant.
RESULTS
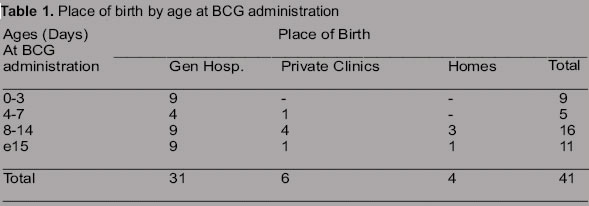
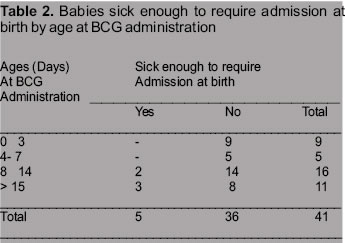
Between the months of November and December 2003, 41 mothers who came to the immunization centre of ABUTH, Zaria were recruited for the study. The ages of their children ranged from 6 to 60 weeks. There were 23 boys and 18 girls. Of the 41 children, 39(95.1%) had BCG scar present and 23(56.1%) of their mothers knew the disease BCG is meant to prevent. The ages at which these children received their BCG by sex is displayed in table 1. It showed that only 9 out of 41 children (22%) received their BCG within the first 3 days of life and 14/ 41 (34.2%) within the first 7 days of life. While most children received BCG in the second week of life, 11 / 41 (26.8%) had theirs after 2 weeks of life. Of the 9 who had BCG in the first 3 days of life, only 3 received BCG on the first day of life i.e., at birth. Out of the 11 who had BCG after 2 weeks of life5, (45.5%) received BCG after the first month of life with 2 of them after the second month of life. Table 2 shows the place of birth of these children by the age at BCG vaccination. All the 9 children who received BCG within the first 3 days of life were born in a General Hospital and only 1 out of the 14(7.1%) who had BCG within the first week of life was born outside a general hospital set up (Private clinic). On the other hand, 9 /27 (33.3%) of those who received BCG after the first week of life were either born in a Private clinic or at home. The difference is however not statistically significant (P>0.05). The distribution of the Mother's educational level, Gestational age at delivery, mode of delivery and birth weight was similar among the various ages at BCG administration. When the question of whether the child was sick enough at birth to require hospital admission was asked, mothers of all children who had BCG within the first week of life said no while 5 of the 27(14.3%) children who had BCG after 2 weeks of life said yes. This difference is also not statistically significant (P>0.05).
DISCUSSION
This study has demonstrated that despite the National Programme of Immunization (NPI) recommendation of administering BCG at birth, about 65.8% of babies in Zaria receive their BCG after the first week of life. Although the official WHO recommendation is a single dose administered any time during infancy, in Nigeria, just like in other developing countries with high transmission rate of tuberculosis, it is important that BCG vaccination be administered early, where possible at birth, before the child comes in contact with the tubercle bacilli. The place of birth and whether a child was sick enough at birth to require hospital admission appears to be an important factor affecting the age at BCG administration. In this study, a child that is born in a general Hospital is more likely to have BCG vaccine administered at birth. In Uganda, Odiit and Amuge 6 also reported that a child born in a health facility was more significantly likely to have BCG administered than a child born at home. This may be explained by the fact that general hospitals are staffed with qualified nurse and midwives. They are therefore likely to advice the mothers on the importance of vaccination and the timing of vaccination. Wood et al 7 reporting on knowledge of the childhood immunization schedules and of contraindications to vaccination by private and public health care providers in Los Angeles showed deficiency in knowledge of the immunization schedule and the appropriate contraindications to vaccinations by private physicians and nurses compared to public physicians and nurses. Most of the private clinics in our environment are staffed with unqualified nurses who are mostly trained on the job by the proprietors of the clinic. The implication of this is that there are lots of missed opportunities to vaccinate children against tuberculosis, leading to low immunization coverage. From the foregoing therefore, there is a need for appropriate health education of the health care providers, particularly those in the private sector with respect to the importance of BCG vaccination and the appropriate timing of such vaccination. In our own environment, these should be extended to the Traditional Birth attendants (TBAs), who are the traditional midwives attending to deliveries at homes.
REFERENCES:
Copyright 2004 - Journal of Community Medicine & Primary Health Care
The following images related to this document are available:Photo images[pc04008t1.jpg] [pc04008t2.jpg] |
| |||||||||

{kind=link}
{kind=link}