 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Adverse Drug Reactions; As a Cause for Admissions to a Children's Hospital Seyed Bahram Mir Saeed Ghazi1, MD; Mojtaba Dibaee* 1, MD; Peyman Salamati2, MD; Ali Akbar Rahbari Manesh1, MD; Hamed Akhlaghi3, MD 1Department of Pediatrics, Tehran University of Medical Sciences,
Tehran, IR Iran Received: 11/6/2006; Code Number: pe07002 Abstract:
Objective: The aim of this study was to investigate the adverse drug reactions
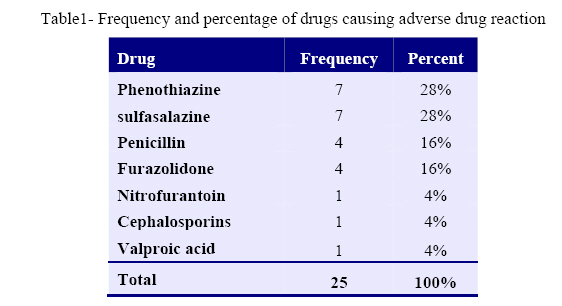
(ADR) in pediatrics and determine the predominant symptoms of adverse drug reactions in children. Key Words: Drug reaction, Side effects, Urticaria, Skin rash, Children Introduction According to the WHO in 1972: an adverse drug reaction (ADR) is a response to a drug which is noxious and unintended, and which occurs at doses normally used in man for the prophylaxis, diagnosis, or therapy of disease, or for the modification of physiological function [1]. A more recent definition, also taking causality assessment into account, defines an ADR as an adverse drug event that is judged to be caused by the drug [2]. Drug-related problems are believed to constitute a substantial health care problem as well as a health care cost. In a review article based on 36 English-language studies, the prevalence of hospital admissions due to adverse drug reactions (ADRs) ranged from 0.2 to 21.7% and the median was 4.9% and the mean was 5.5% [3]. In a recent review based on 39 prospective studies from hospitals in the United States, the overall incidence of serious adverse drug reactions was 6.7%, and fatal ADRs was 0.3% [4]. In a national prospective cross-sectional study in 62 medical departments of 33 hospitals in France, 3.2% of admissions were caused by ADRs [5]. In two Swedish studies, undertake about 20 years ago, 5.6 and 8.6 percent of the patients were admitted to a clinic of internal medicine due to adverse drug effects [6]. The purpose of the present study was to determine the current occurrence and pattern of adverse drug reactions as a cause for acute admission into a pediatric clinic as a background to future interventional studies in order to decrease the occurrence of ADRs. Material & Methods This case series study was carried out at the Bahrami Children's Hospital affiliated to Tehran University of Medical Sciences. Data collection was undertaken for 8 years during the period 1998 to 2005. Information was taken from the patient medical records, concerning associated symptoms, use of drugs, associated diseases, the result of the medical investigation obtained by the medically trained staff and a questionnaire to be filled which was specifically designed for this study. The term intoxication was defined as an intentional or accidental poisoning. Type A adverse effects, are those effects that are related to the known pharmacological effects of the drug and that are dosage-related. Type B, are those effects that are often allergic or idiosyncratic reactions characteristically occurring in only a minority of patients and usually unrelated to dosage. These reactions are typically unexpected, unpredictable and often serious. A serious adverse drug reaction was classified as a reaction, which is fatal, life threatening, disabling or incapacitating. Statistical analyses were performed with chisquare tests. SPSS 12.0 was used to analyze the data. Findings During a 8-years observation period, a total of 25 patients (16 males, 9 females) were admitted to the Bahrami Children’s Hospital with the diagnosis of ADR. The average age was 4.6 ± 3.7 years with a range of 1 month to 14 years. Symptoms of adverse drug reactions were observed 12.6 (±14.3) days after initiation of the drug intake (between 3 and 69 days). Skin rash was seen in all patients. 56% of patients had maculopapular, 16% urticarial and 28% both maculopapular and urticarial rashes. Most patients had a temperature between 37.3°C and 39.9°C (76%). Only one patient had a temperature of 40°C. One hepatosplenomegaly and one wheeze reaction was reported in our study. After rash, the most common ADR was arthralgia which was reported in 44% of our patients. In laboratory data, 12% of patients had eosinophilia (absolute count of eosinophile >450), 8% had thrombocytopenia (platelet > 450000) and 20% had thrombocytosis (platelet <150000). Predominant abnormal laboratory data was high erythrocyte sedimentation rate (ESR > 25) seen in 40% of patients. The most common culprit drugs were phenothiazine and sulfasalazine (each of them seen in 28% of patients) followed by penicillin (16%), furazolidone (16%), nitrofurantoin (4%), cephalosporins (4%) and valproic acid (4%) (Table 1). In 28% of patients poly-pharmacy was responsible for ADR. Discussion Adverse drug reactions represent a significant health problem [7]. Monitoring of ADR in the clinic is crucial in order to increase the quality of life for the patients and to reduce morbidity and related health care costs. It is also important as a quality assessment [8]. In the present study, all ADRs were rated as pharmacological reactions (type A). The most common symptom was skin rash followed by arthralgia, both of which are not specific for ADRs. Although it is difficult to prevent type B reactions, it has been suggested that at least half of the pharmacological (type A) reactions could be prevented [6, 9, 11], some large studies even suggest that more than 70% of the ADRs could be preventable [10]. About 30 years ago, a prospective laborintense drug surveillance study was performed in the Department of Medicine at the Karolinska University Hospital.6 This study showed that 5.6% of patients were admitted due to probable or certain ADRs. Intoxication with prescription drugs was the reason for admission in 3.5%. A recent large prospective study of ADR-associated admissions in UK found a similar percentage of ADR-related admissions (6.5%). Improvement of drug safety is important not only in terms of patient morbidity and mortality but also in economic terms. If only a fraction of all preventable adverse drug reactions could be avoided, it would result in a significant reduction in morbidity and health care costs. Many of the type A reactions might be avoided by taking various measures. Among them, a more thorough collection and registration of the medication history, a computer-based prescription has also been suggested in addition to better systems for monitoring drug therapy and reporting adverse drug reactions [12-15]. It has also been recommended that treatment decision-making should be shared with the patients and that efforts should be made to improve the communication process between doctors and patients [16]. Preventive measures, such as monitoring drug therapy and providing increased education and advice to the prescribers may reduce the patient's problem with ADRs. But the different strategies must be tested under field conditions. Methods for continuous ADR surveillance should be important parts of quality assurance programmes in health care. Conclusion ADR is one of the most common reasons for acute admission to hospital. Most of the ADRs are due to the pharmacological profile of the drug (type A) and thus predictable although not always preventable. Awareness of the problem, observation of poly-pharmacy and potential drugdrug interactions, and continuous re-evaluation of the ongoing individual pharmacotherapy are important, especially in children in order to reduce ARDs. References
Copyright 2007 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe07002t1.jpg] |
| |||||||||

{kind=link}