 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Prevalence and Severity of Anemia in Pediatric Hemodialysis Patients; A Single Center Study Afshin Azhir* 1, MD; Jafar Nasiri1, MD; Alaleh Ghasari 1, MD 1Department of Pediatrics, Isfahan University of Medical Sciences,
Isfahan, IR Iran | Received: 11/6/2006; Code Number: pe07006 Abstract Objective: To determine the prevalence and severity of anemia in children
and adolescents on chronic hemodialysis and to identify independent predictor
for anemia in children on hemodialysis. Key Words: Hemodialysis, Anemia, Prevalence, Erythropoietin, Parathyroid hormone Introduction Anemia is a major complication of end-stage renal disease (ESRD) in children
[1]. When severe, it is associated with cardiovascular dysfunction, cardiomyopathy,
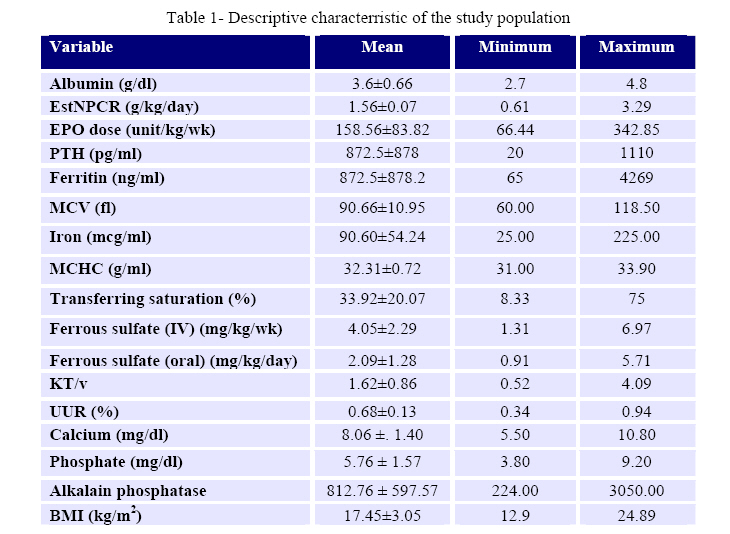
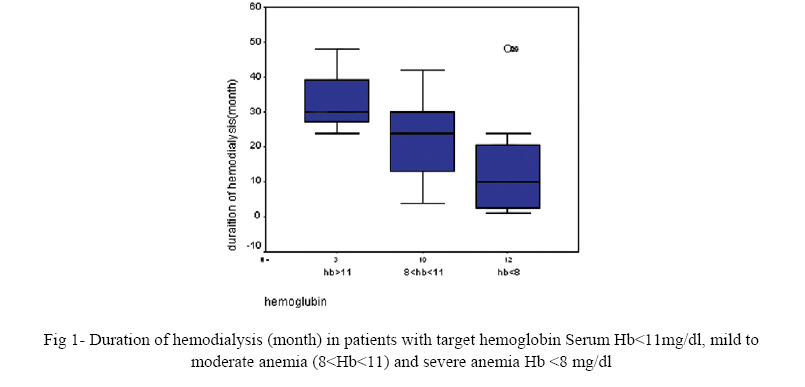
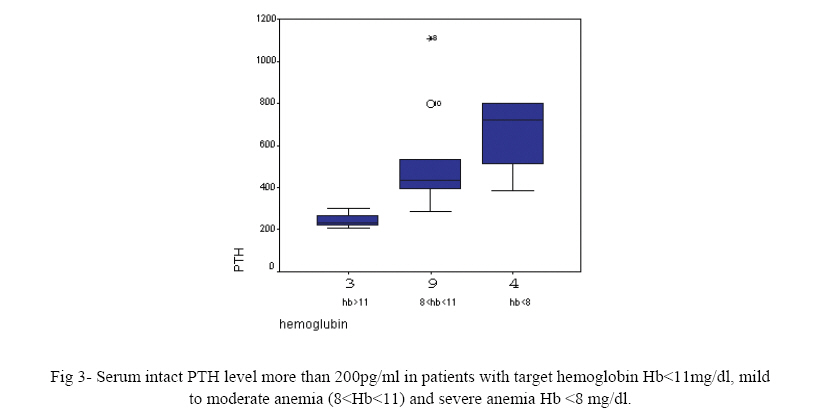
and death [2] Correction of anemia in children with ESRD improves cardiac The major cause of anemia in patients with chronic kidney disease and end-stage renal disease (ESRD) is erythropoietin (EPO) deficiency, resulting from its decreased production from the kidneys [2]. The remarkable development and subsequent introduction of recombinant human erythropoietin (rHuEPO) in 1989 made it possible to safely and effectively treat the anemia of renal insufficiency and practically eliminate the need for repeated transfusion [5]. Despite the advances in dialysis care and the use of erythropoietin, anemia continues to be a clinical problem seen in patients with ESRD [3]. It was believed that iron deficiency was the major predictor of EPO hyporesponsiveness [6]. Despite the extensive use of erythropoietin and iron supplements, over one third of children aged between 12 to <18 maintained on chronic hemodialysis have a mean hemoglobin of less than 11 g/dL [3]. Other factors that have been shown to influence the response to rHuEPO in adult and pediatric patients on dialysis include dosage, route of administration, acute or chronic infection and aluminum intoxication[1]. Refractory anemia appears to be more common in those patients on dialysis who also suffer from protein-energy malnutrition (PEM) or inflammation[6]. Secondary hyperparathyroidism contributes to resistance of rHuEPO in adults [1]. Craig et al showed when serum PTH levels were markedly elevated in pediatric patients, response to rHuEPO will be poor [1]. The objectives of this study were 1) to determine the prevalence and severity of anemia in children and adolescents on chronic hemodialysis, 2) to identify independent predictors for anemia in children on hemodialysis. Material & Methods A cross sectional study was performed between September 2005 and January 2006 at the Isfehan medical University, department of pediatrics with the Permission of the Ministry of Education. The study population consisted of 25 patients on chronic hemodialysis from pediatric hemodialysis centers in Isfahan, Iran. All the patient- specific parameters were recorded, including age, gender, pre and post dialysis body weight, height, body mass index (BMI), cause of ESRD, duration of dialysis (6 months vs.6 months or longer), and the access type used dialysis. Blood studies were performed immediately pre dialysis. Hemoglobin level, hematocrite, reticolocyte count, indirect bilirubin, lactic dehydrogenize, direct coomb’s test, serum urea nitrogen, serum iron, ferritin, transferring, serum calcium, phosphate, intact parathyroid hormone (PTH), C-reactive protein, albumin and alkaline phosphates were measured. Another blood sample for serum urea nitrogen was taken 30 minute after dialysis session. Data on patient rHuEPO dose (unit/kg/week), and oral iron (mg/kg) or administration of intravenous iron (mg/kg/week) were obtained from dialysis charts. All routine laboratories measurements were performed by Cobas Mira -S using automated methods. Serum intact PTH and ferritin (ng/mL) were measured by a chemilumineescence immunoassay. Serum CRP was obtained to indicate the presence of an inflammation state. Body mass index (BMI) was calculated as weight (kg)/height (m2) [2]. Anemia was defined as a hemoglobin value less than 11g/dl and severe anemia defined as a hemoglobin value less than 8g/dl. Iron deficiency was defined as ferritin ≤100ng/dL or the percentage transferring saturation less than 20% and mean corpuscular volume (MCV) <75fl. Megaloblastic anemia was defined as MCV>100 fl and LDH>190 and retic<1%. Serum intact PTH >200 pg/ml was considered as high turn over bone disease secondary to hyperparathyroidism. Kt/v values were calculated using the Daugridas 2 formula. Adequate dialysis clearance was defined as Kt/v≥1.2 and UUR≥65%. Estimated normalized protein catabolic rate (EstNPCR) was calculated by Borch equation to estimate the daily protein intake. EstNPCR <0.8 g/kg/day was defined as malnutrition. The results were analyzed using the Statistical Package for Social Sciences (SPSS 11.5) program and expressed as mean and standard deviation. Statistical analysis of data was performed by Spearman and Pearson tests to show correlation between anemia and other variables. Differences of P<0.05 were considered to be statistically significant. Findings The study group was composed of patients aged between 7-20 years (3 patients were less than 12 years and 22 were more than 12 years). The mean age of patients on hemodialysis was 15.5 ±3.7 years. There was 13 females (52%) and 11 males (48%). Mean duration of hemodialysis was 20.4 ±15.2 months (1-48 months). Hemodialysis access was by arteriovenous graft (1 patient), AV fistula (15 patients), or permanent right arterial catheter (8 patientss), temporaray right arterial catheter (1 patient). Five patients (20%) had a pervious history of transplantation. C-reactive protein was positive in 5 patients. The disorders causing ESRD in the study group included nephronophthesis (8%) posterior urethral valve (8%), Alport syndrome (4%) systemic lupus erythromatus (4%), henochschonlein purpura (4%), reflux (8%), renal dysplasia (4%), single kidney and post-traumatic nephrectomy (4%) spinal injury (4%) glomerulonephritis (16%) focal segmental glomerulosclerosis (8%) and in 6 patients (24%) the etiology was unknown. The mean hemoglobin was 8.49±3.02 g/L (5.30-17.30) (Table 1). Twenty-two patients (88%) had hemoglobin value less than 11 g/dl (anemia) and 48% (12 patients) had hemoglobin value less than 8 g/dl (severe anemia). There was evidence of hemolytic anemia (LDH > 300,positive coomb’s test) in two patients. In 4 patients (20%) MCV was more than 100 fL (megaloblastic anemia). There was no correlation between age and hemoglobin (r=0.22, P=0.3) and there was also no correlation between gender and hemoglobin (r=-0.24, P=0.2). Anemia was more common among children that were on dialysis for less than 6 months (6 of 6 patients) (100%) compared to children on dialysis for 6 months or longer (16 of 19 patients) (83%). Anemia was also more severe in patients who were on dialysis for less than 6 months (5 of 6 patients) (83%) compared to children on dialysis for 6 months or longer (7 of 16 patients) (43%). Therefore, there was an inverse relation between the severity of anemia and duration of hemodialysis (P=0.019, r=-0.46) (Fig 1). Nearly all children (92%) were treated with erythropoietin with no differences between the routes of administration. Children with more severe anemia received slightly higher dose of erythropoietin (P=0.09, r=0.202). There was no correlation between erythropoietin dose and hemoglobin level (r=-0.180, P=0.4). Children with anemia received higher weekly erythropoietin doses (167.19±86.61 units/kg/week) versus children with target hemoglobin level (101.03±19.36 units/kg/week), (P=0.2); and children with severe anemia received higher weekly erythropoietin (161.85± 73.36 units/kg/ week) versus children with mild to moderate anemia (173.71± 104.88 units/kg/ wk) (P=0.4). One of 31% of anemic children had mean transferrin saturation (TSAT) less than 20%. Absolute iron deficiency (defined as a TSAT of less than 20% and a ferritin less than 100 ng/mL) was only seen in one patient. Five patients (20%) were not treated with iron preparations. Approximately 24% of the children were treated with intravenous iron and their mean iron dose was 4.05±2.29 and 56% of them were treated with oral preparations and their mean iron dose was 2.09±1.28. There was no correlation between intravenous iron dose and hemoglobin level (r=0.66, P=0.1). There was also no correlation between oral iron dose and hemoglobin level (r=0.36, P=0.2). There was no significant difference between oral and intravenous routes for iron administration in anemic patients. Treatment with oral iron was not different according to dosages prescribed in the anemic children in spite of severity. Although there was no information on patients' compliance. The calculated single-pool Kt/V of 1.2 or greater defined dialysis adequacy. The mean Kt/V values were (1.62±0.86). Dialysis clearance was inadequate in 5 patients (20%). There was no correlation between dialysis clearance and hemo- globin level (r=0.13, P=0.5). AV fistula was more commonly used as access in anemic children. The URR of 0.65 or greater was defined another parameter for dialysis adequacy. The mean URR values were (0.68±0.13). According to URR values dialysis clearance was inadequate in 9 patients, however, only in 5 of them the Kt/V values were less than 1.2. There was no significant difference between URR values in patients with Hb<8 (severe anemia) and 11 Intact PTH level was more than 200 pg/ml in 16 patients (66%) and more than 400 pg/ml in 9 patients (37.5%). Finally, there was no correlation between intact PTH level and hemoglobin level (p=0.336,r=-0.205) but there was a reverse correlation between intact PTH level>200 pg/ml and hemoglobin level (r=-0.505, P=0.046) (Fig 3). Discussion Despite the extensive use of erythropoietin and prescribed iron supplements, over 80% of children maintained on chronic hemodialysis had a mean hemoglobin of less than 11 g/dL. Patients new to dialysis (treated less than 6 months) were more anemic. The degree of anemia prior to the onset of dialysis may account for these findings the data set. Lower serum albumin was related to the anemia. There was a reverse correlation between intact PTH level>200 pg/ml and hemoglobin level. Frankenfield et al showed that 37% (160/435) of HD patients aged between 12 and less than 18 years were anemic in the National 2001 ESRD Clinical Performance Measures Project [3]. Fadrowski et al demonstrated that more than onethird of pediatric patients on dialysis were anemic during the project years of 2000 and 2001 [7]. The 2001 North American Pediatric Renal Transplant Cooperative Study annual report showed that 63% of 1855 pediatric patients on chronic dialysis who were receiving rHuEPO at 6 months of dialysis had hematocrit values of ≤33% (≤11 g/dL) [8]. In our study more than 80% of patients were anemic. The recommended starting dose of rHuEPO is 50-150 U/kg given three times weekly [2]. Our patients received a mean weekly rHuEPO doses of 158 U/kg, these doses were significantly higher than those received by adults. Fadrowski et al showed that an increase in age and dialysis for less than 6 months were 2 factors that enhanced anemia [8]. There was no coorelation between age, gender and anemia in our study but patients new to dialysis (treated less than 6 months) were more anemic. Some patients did not respond to rHuEPO therapy even if high doses were used. The main reason for EPO resistance is iron depletion or insufficient access to iron storage pools [9]. Almost all of our patients had iron supplements. There are no standards for iron adequacy in children on hemodialysis. Iron adequacy in adult dialysis patients has been defined as a serum ferritin concentration>100 ng/ml and percentage transferrin saturation of >20% [10]. Serum ferritin>10ng/ml and precentage transferrin saturation as low as 7% are considered normal for healty children [11]. Serum ferritin > 40ng/ml has been reported to be adequate in children on dialysis [12]. According to the protocol of adult on dialysis only one of our patients had iron defeciency anemia (ferritin=65 ng/ml, TSAT=17.6%) but no one had TSAT<7% and ferritin<40 ng/ml. Serum ferritin level more than 800 ng/dl is belived to be an indication at heavy iron overload [9]. Serum ferritin level were more than 800 ng/dl in 48% of our patients. Megaloblastic anemia (MCV>100 fl) was seen in 4 patients (16%) and in all of them the serum albumin was less than 3.5mg/dl. We did not measure the serum folate and vitamin B12 level in these patients. There was evidence of hemolytic anemia (LDH> 300, positive coomb’s test) in two anemic patients. The platelet count was normal in these two cases. Insufficient dialysis is associated with significant clinical morbidity, an increased risk of mortality, and it also contributes to anemia [13, 14]. Frankenfield et al showed that dialysis clearance no longer appeared to be an important factor accounting for the anemia in pediatric patients on hemodialysis [3]. The mean dialysis adequacy (Kt/V 1.62±.86) for our children on dialysis exceeded the K/DOQI clearance guidelines for adult hemodialysis patients (Kt/V ≥1.2). Although, dialysis clearance was inadequate in 5 patients (20%), there was no correlation between dialysis clearance and hemoglobin level in this study. Fistula access has been considered the optimum choice for hemodialysis management [15]. In our study, 16 patients (60%) on dialysis had on AV fistula access. However, only 25% of them had Kt/V values < 1.2 but 81% of them were anemic. Whether the higher clearances achieved by using a fistula access would really affect anemia and other ESRD-related morbidity in children maintained on chronic hemodialysis has yet to be shown. Severe secondary hyperparathyroidism appears to be an important factor in the severity of anemia in children with chronic renal failure [1]. PTH may be a direct inhibitor of endogenous erythropoitin production [16]. Another mode of action of PTH in ESRD is an increase in red blood cell osmotic fragility, leading to a decrease in red blood cell survival time [17]. Synthetic PTH or serum from hyperparathyroid patients has been reported to inhibit red blood cell precursours in vitro in some studies [18]. Likewise, hyperparathyroidism may also affect anemia by causing bone marrow fibrosis,which reduces the available space for erythroid-forming units[19]. A serum PTH level at >200 pg/ml has been shown previously to be strongly predictive of osteitis fibrosa in children [20]. PTH effect on erythropoisis can be overcome by higher doses of rHuEPO. PTH level at >200 pg/ml was seen in more than half of our patients and more than one third of them had PTH level at >400pg/ml. There was a reverse correlation between intact PTH level at >200 pg/ml and hemoglobin level in our study. Low serum albumin and anemia were related in adult patients maintained on hemodialysis but in the context of inadequate dialysis clearance [13]. Frankenfield et al raised the possibility that two variables, anemia and albumin, are associated independently from dialysis clearance in pediatric patients and support the view that poor nutrition may be an additional factor for anemia [3]. Improving nutritional state in patients on dialysis may improve anemia and lead to a lower requirement at EPO. In a meta-analysis by Hurot et al, L-carnitine administrations, used to improve nutritional state, was associated with improved hemoglobin level, decreased EPO dose and EPO resistance in anemic patients on dialysis [21]. Nearly half of our patients were hypoalbuminemic (albumin<3.5g/dl) and EstNPCR was less than 0.8 in one/forth of them. There was also correlation between serum albumin level and hemoglobin level in this study. Several previous studies reported an association between anemia and inflammation in patients on dialysis, reflected by a high serum concentration of CRP [22]. Moreover, IL-1 and TNF-α have been shown to inhibit EPO production in vitro and to have a suppressive effect on erythropoiesis [23, 24]. Uptake of iron is lower than normal in inflammation [25]. Serum level of ferritin, a marker of iron stores and also a positive acute-phase reactant, have been shown to be paradoxically high in patients with ESRD with refractory anemia [26, 27]. Increased ferritin production may prevent iron delivery to erythrocyte precursors [26]. Finally, Patients with inflammation may be more prone to gastrointestinal bleeding[25]. In this study, inflammation existed in 5 patients in wich serum ferritin was >1000 ng/ml in 3 of them. Conclusion Pediatric patients on chronic hemodialysis in Isfehan may be undertreated for anemia despite the extensive use of rHuEPO supplementation. We found this to be especially true for patients new on hemodialysis (less than 6 months) and low albumin. Iron deficency was not the main cause of anemia. Severe hyperparathyroidism, malnutrition, and inflammation, should be considered as other causes of anemia in this study. The results of this study indicate the need for continued improvement in the management of anemia in children undergoing chronic hemodialysis. References
Copyright 2007 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe07006f2.jpg] [pe07006f1.jpg] [pe07006t1.jpg] [pe07006f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}