 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Exercise and Diabetes Type 1 Recommendations, Safety Ramin Kordi *1, MD, PhD; Ali Rabbani2 MD 1Center for Sports Medicine. University of Nottinghamm, UK Sports
Medicine Research Center, Tehran University of Medical Sciences, Tehran, IR
Iran Received: 10/4/06; Code Number: pe07010 Abstract Type 1 diabetic subjects without any complications and with a good control
could participate in all
levels of sports activities, both recreational and professional. But, there
are some limitations for
subjects who have chronic side effects of diabetes. A detail pre-participation
physical examination
is needed to find out these complications. All diabetics should be encouraged
to perform suitable
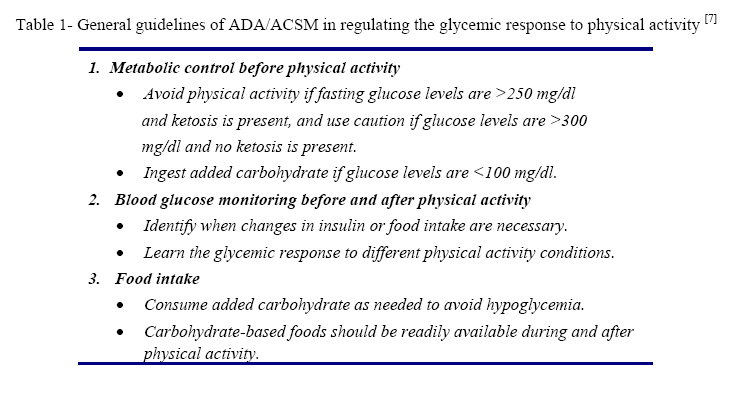
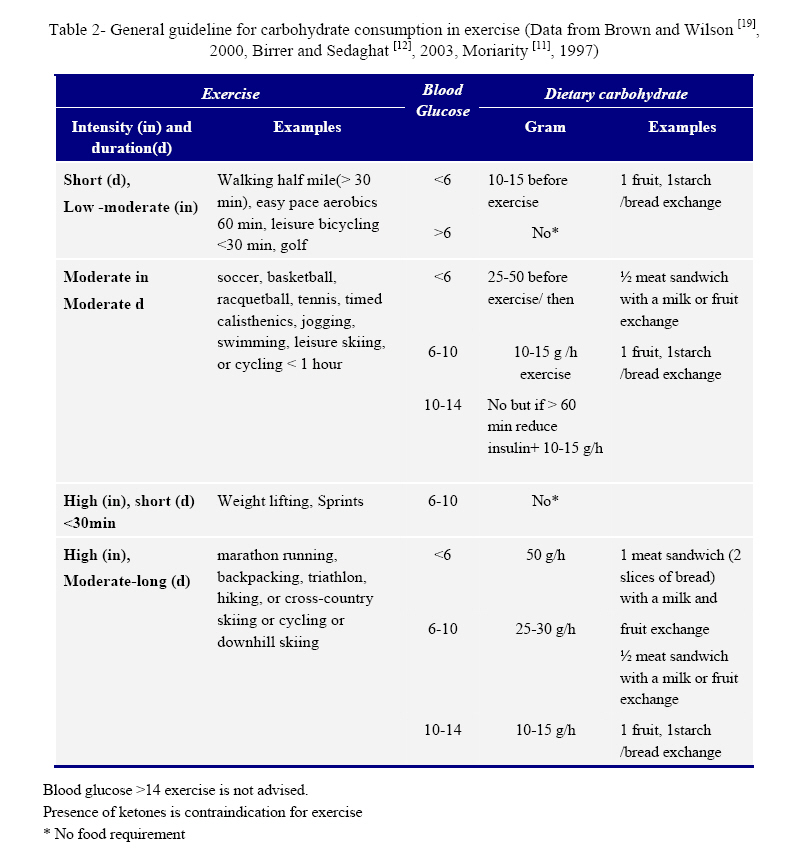
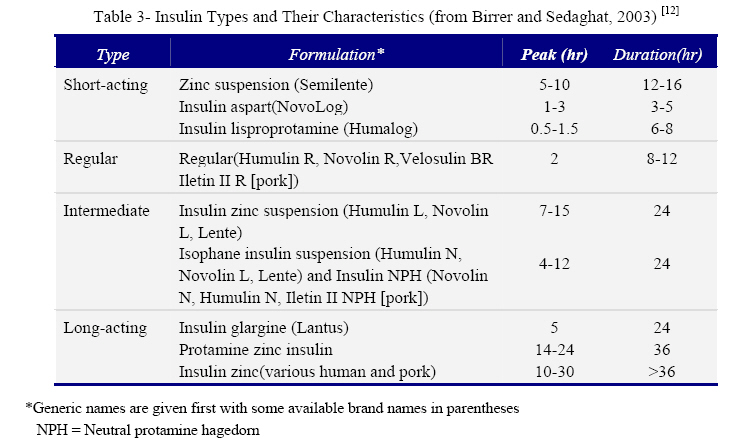
exercise and sports. Key Words: Diabetes, Exercise, Hyperglycemia, Hypoglycemia, Sports, Blood glucose Introduction The worldwide prevalence of diabetes is increasing [1]. Diabetes is known as an epidemic disease [2]. It is suggested, that the number of athletes with diabetes at all levels, recreational and professional is increasing [3]. There are a number of Olympic gold medalists and high level professional athletes who have diabetes type 1 [4,5]. But, there are not enough research, papers and texts in this field [1]. Also, there are few published guidelines on physical activity and diabetes, only joint position statement of American College of Sports Medicine (ACSM) and American Diabetes Association (ADA) [6, 7]. There are no popular outline from the International Sports Medicine Federation (FIMS) available [8,1]. These recommendations also are quite generally advised [9]. Paula Harper, the president of the International Diabetics Athletes association, has completed 31 marathons, 1 ultra marathon, 5 triathlons and 6 century (100 plus miles) bicycle races. She said, there is not enough information available which could help diabetics to do exercise and sports safely [4]. This review, discusses the required recommendations regarding patients with diabetes type 1 who want to participate in sports and exercise safely. Diabetes type 1 Diabetes is a group of chronic metabolic disorders which is recognized by increased blood glucose due to reduced insulin secretion and/or reduced insulin action [10]. Diabetes falls into two main groups, type 1 and 2. Of all diabetics, 10% have type 1 diabetes or insulin-dependent diabetes mellitus (IDDM) [1]. In the type 1 diabetes, dysfunction of pancreatic beta-cells leads to a deficiency of insulin production. About half of type 1 patients are younger than 20. Prevalence in this range of ages is about 2.5 to 3.5 per 1,000 [6]. The aim of treatment of IDDM, is keeping insulin levels normal, prevention of micro and macrovascular complications[1]. It is demonstrated that in IDDM patients' tight glucose control prevents the development and progression of diabetic complications [11]. Diabetics with type 1, need insulin for treatment. Several insulin dosage regimes could be used by diabetics. Regimes may be standard (two injections of mixed short and intermediate insulins), intensive (three or more injections/day), extended (glargine or insulin zinc suspension for basal needs plus lispro for meals), or continuous infusion by pump [12]. Traditionally, regimens are included of basal insulin which is 50% of the daily insulin dose. Basal insulin consists of intermediate or long acting insulin injected once or twice a day in the morning and evening. The rest of the daily dose consists of fast acting regular insulin injected before breakfast, lunch, and sometimes dinner to reduce the glycemic effects of meals [1]. Positive effects of exercise The American Diabetes Association and the American College of Sports Medicine state that, young patients with good metabolic control can safely participate in most activities. Also, they confirm that the middle-aged and older patients should be encouraged to increase their physical activity [13]. Physical activity and exercise can be beneficial in controlling serum lipoprotein, reducing blood pressure, and improving cardiovascular fitness, psychological well being and social interaction and reaction [1,7,14]. Exercise and training help patients to feel that they are in control of their condition [12]. To gain these beneficial effects, patients should be encouraged to do sports and exercise in both recreational and competitive levels [7, 10]. Effects on diabetic controls Several studies using fasting plasma glucose and HbA1c failed to show that exercise training could improve glycemic control in the patients with diabetes type 1 [15,16]. However, Schneider et al [16] report that some patients who seriously adjust their insulin and manage their blood glucose levels could improve their diabetes control. They suggest that, exercise can improve glycemic control in type 1 diabetes with the effort of patients and doctors; however, this would be very difficult to achieve [2, 16]. Insulin in athletes Insulin is classified as an anabolic agent and is in the prohibited classes of substances by International Olympic Committee. It is only permitted to treat athletes with certified insulin-dependent diabetes. The term "insulin-dependent" is defined as diabetics who need insulin to be treated, all patients with type 1 and some patients with type 2[17]. Most patients with IDDM need between 0.5 and 1.0 U/kg/day of insulin. Regular exercise increases insulin sensitivity and decreases insulin requirements in the type 1 diabetics [11,16]. As a result, in athletes, required insulin doses are lower, between 0.2 and 0.6 U/kg/day [1]. Pre-participation physical examination Diabetics need a detailed medical evaluation with appropriate diagnostic studies before starting exercise and sports. Any macro- and microvascular complications should be detected carefully. On the base of this finding; every patient should have his or her individual exercise recommendations [7, 12]. Medical history and physical examination should be focused on the symptoms and signs of diseases affecting the heart and blood vessels, such as the eyes, the kidneys, the feet, and the nervous system. The patients who are at high risk for cardiovascular disease (age >35 years, type 1 diabetes for >15 years, have macro-or micro vascular disease) may need a stress exercise test [7]. Diabetics who have proliferative retinopathy should avoid anaerobic exercise and physical activities that involves straining, jarring, or Valsalva-like maneuvers7. There is no obvious reason to limit low to moderate intensity exercise in diabetics with nephropathy. But, high intensity or strenuous exercise should probably be limited in these groups unless blood pressure is carefully monitored during exercise. Peripheral neuropathy may cause loss of protective sensation in the feet. Therefore weight bearing exercise should be limited in severe cases [7, 12]. Nutritional and insulin adjustment Blood insulin level decreases shortly after starting exercise in the normal people. In contrast, it may stay the same or increase during exercise in the patient with IDDM. Insulin level in these patients, is determined mainly by the amount and timing of the last injection [15,18,19]. To avoid side effects of high insulin level such as hypoglycemia, insulin should be decreased or more carbohydrates consumed[2]. However, it may be reasonable to mimic the physiological pattern by reduction of insulin dose before exercise, instead of increasing food intake [20]. To follow this approach, in advance the patients should anticipate detailed characteristics of the exercise such as duration, intensity, time of the day, time from the last meal and insulin activity during exercise; also, they should know their metabolic response to different kinds of physical activity and the characteristics of used insulin such as dosage, half-life and timing of effect. On the base of this data insulin dose could be adjusted [7,11,15,19,20]. In practice, management of diabetic athletes is not strait forward. For example, theoretically if the intensity and duration of the activity were the same in every session, calculation of insulin and food adjustment would be easier. But, it is too difficult to have a similar physical activity all the time. Unplanned situations are frequently happening [4]. In unexpected exercise, when insulin dose is not reduced, the only option is consuming carbohydrate before and during exercise [15]. Insulin regimens and formulation are different among individuals with IDDM [15]. The physiological response to exercise in diabetics depends on several factors such as the type of diabetes, degree of control, bioavailability of insulin, diet, and fitness level [12]. Also, needs for insulin is different in the different hours of the day [15]. As a result, each patient responds differently to exercise, but the recommendations for insulin and food adjustment could be used as a general guideline [14]. On the base of these recommendations, each patient should find optimal approach for his/her situation [14, 20]. ADA/ACSM state that the rigid recommendation of consumption of carbohydrate supplement on the base of anticipated intensity and duration of physical activity is not recommended. They recommend that other data should be considered such as blood glucose level at the beginning of physical activity, the previously measured metabolic response to physical activity, and the patient's insulin therapy. General guidelines of ADA/ACSM in regulating the glycemic response to physical activity are summarized in table 1 [7]. Insulin adjustment Daily insulin requirement may decrease with any kind of physical activity even activities such as household chores [1]. If physical activity is less than 20-30 minutes duration; usually, insulin reduction is not necessary. For longer physical activities, insulin should be reduced by 14-50%. The exact amount of reduction depends on the intensity, duration of exercise and individual response [15,19]. For very high intensity and prolonged physical activities such as marathons and triathlons reduced dose may be as high as 70- 90% or even 100% [1]. The duration of exercise indicates that which insulin dose should be decreased. Generally, the insulin dose which has high activity during exercise should be reduced [19]. For example, exercising 1 hour in the morning needs a 25% reduction in before-breakfast regular insulin for moderate activity, and 35% to 50% reduction for vigorous or sustained activity or for afternoon exercise, the longer-acting insulin (NPH or Lente) before-breakfast dose should be reduced as for morning activity. For evening exercise, patients should reduce both regular and longer-acting insulin before the supper dose [12]. Blood insulin level, could be roughly estimated by measuring blood glucose level [15]. Ideally, blood glucose level should be monitored each morning, before and after exercise and before and after meals. Athletes involved in potentially unsafe activities such as scuba diving should check blood glucose at 90, 30 and 5 minutes before exercise [1,15]. Levels of glucose before and after exercise show the response of the athletes to the insulin, nutritional adjustment and the physical activity. Every diabetic athlete on the base of his/her response should find his or her own routine. This could be achieved mainly by try and error [4,5]. Before starting exercise, patients must have a good control at their blood sugar. They should avoid exercise when they are metabolically unstable. If the blood glucose before exercise is above 14 mmol/l (250 mg/dl) and there is (1-2+) ketosis in the urinalysis or blood glucose is more than17 mmol/l (300 mg/dl) exercise must be avoided. On the other hand, if blood glucose is lower than 5.5-6.0 mmol/l (100 mg/dl) the subject must ingest extra carbohydrate and avoid vigorous or prolonged exercise [1,7,20]. Using and abusing drugs by diabetic athletes which could affect blood glucose and diabetic control should be avoided, such as anabolic steroids and stimulants which may worsen hyperglycemia. During some periods of reduction activity such as off season, holidays or recovery from injury, insulin requirements may be increased [1]. The recommendations of the FIMS The recommendations of the FIMS are rather general. They recommend that insulin doses should be decreased by 20% or food intake should adequately be increased before starting exercise. Also, they advise to consume a small carbohydrate snack 30 minutes before exercise to prevent hypoglycemia. Moreover, during more prolonged exercise, 10 g of carbohydrate snack (fruit, fruit juice, or soft drink) should be taken for each 30 minutes of exercise [8]. Site of injection During exercise many factors might increase insulin absorption such as increased blood flow to the site of insulin injection, increased ambient temperature and massage to the injected site which may all lead to hypoglycemia. Koivisto [21] showed that exercise increases the absorption of insulin when injected in the thigh immediately before leg exercise. He suggested that injection of insulin to the non-exercising part of the body might prevent exercise induced hypoglycemia. However later, it was shown that this approach could not effectively prevent hypoglycemia; especially when insulin was injected half an hour or more before starting the exercise [15,20]. It is reported that there is about 15% variation in insulin absorption rate in a person from day to day. Also, insulin is absorbed from the abdomen site quite more rapidly than the thigh site. Therefore changing the site of injection could make it more difficult to calculate the required insulin [15]. It is recommended to have a routine site and technique of injection [1]. It is sensible to avoid injecting into the active extremity [12]. Abdomen may be a good site, because it is probably less affected during exercise and is easily accessible. The abdomen is the most common injection site used by athletes [1]. Other factors such as increased ambient temperature and massage to the injected site may also increase the absorption of insulin [1,15] which should be considered in insulin adjustment. Also, intramuscular injection of insulin could lead to hypoglycemia during exercise and should be avoided [1,16]. Insulin pump Intensive insulin therapy (multiple daily insulin injection or insulin infusion pumps) may lead to better overall blood glucose control [9]. Provides more flexibility in food consumption and making appropriate insulin dose adjustments for various activities [7,14]. However, Using insulin pump needs more education and may increase the risk of infections and irritation in the infusion site and may lead to displacement of the pump [9,22]. Pump is increasingly used by elite diabetic athletes [1]. Nutritional requirement Nutritional recommendations for training and competitions for diabetic athletes are the same as non-diabetic athletes [23]. Diabetic athletes should generally be advised to adjust their insulin dose without changing their eating pattern[19]. The intensity and duration of exercise shows the amount of extra food needed to be consumed by athlete. Pre-exercise blood glucose shows the timing of food ingestion [16]. With proper adjustment of insulin, the glucose needs of diabetics are the same as non-diabetics [15,19]. The amount of needed glucose varies from person to person but general recommendations are available for everyone (table 2). Each person shouldfrequently monitor his/her blood glucose and based on the response to the exercise and food consumption find his/her own appropriate method. The most suitable approach is by trial and error [19]. Preferred sports and contraindications ADA/ACSM state that people with type 1 diabetes who don't have any complications and that have a good blood glucose control can perform all levels of physical activity, including recreational activities and competitive professional sports [7]. However all the ADA, ACSM and FIMS confirm that aerobic activities such as brisk walking, cycling, jogging or running at moderate intensity are the recommended types of exercise [7, 8]. Recommendations to diabetic athletes for training exercise and sports are the same as nondiabetics and should include a proper warm-up and cool-down period [7]. It may be acceptable for young patients to do high resistance exercise using weights, but not for older individuals or those who have long-standing diabetes. Moderate weight training programs using light weights and high repetitions can be safe in nearly all patients with diabetes [7, 8]. Some sports are restricted for patients with diabetes. The sports which are totally restricted are boxing, flying, motor car racing and paragliding. There are some restrictions in some other sports such as ballooning, gliding, motorcycle racing, parachuting, power boat racing, rowing and underwater swimming [15]. All patients with diabetes should have the opportunity to do exercise and sports and be benefitted from the important positive effects of exercise [7]. Effects of training Diabetics show the similar biochemistry changes in the aerobic and non-aerobic fluxes as control. It is reported that maximum oxygen consumption is lower among diabetics but it could increase by exercise. Also, muscle glycogen is quite lower in the diabetics but glycogen synthesis and store are enhanced by training [16]. Risks of exercise The three major risks of exercise in patients with type 1 diabetes are hypoglycemia, hyperglycemia and chronic degenerative complications [12]. Hypoglycemia Hypoglycemia is the most common problem in the athletes with IDDM [19]. It may occur during, immediately after or several hours after exercise, mainly 12-14 hours or even longer [15, 24]. Several reasons could cause hypoglycemia such as hyperinsulinemia during exercise, high intensity and high duration exercise (>30-60 minutes), more than 3 hours interval between the last meal and exercise and not using a snack before and during exercise [15]. Hyperinsulinemia could be due to exercise at the time in which the activity of insulin is maximum, increase absorption of insulin facilitated by exercise of the injected limb and/or exercise in hot weather [10, 15, 20]. Patients should know when the used insulin is at the peak level activity (table 3). Exercise at this period is associated with high risk of hypoglycemia [2]. Underestimation of insulin dose is quite common among diabetics [15]. Normally, the central nervous system uses only glucose as fuel. Therefore, blood glucose level is well controlled in different situations such as sports and exercise activities. But hypoglycemia could also happen during a prolonged exercise in normal people [7]. Even with a very good control, hypoglycemia can still occur in the diabetic athletes during exercise [1]. Hypoglycemia during exercise is commonly mild and can be treated easily [12]. However, if symptoms are ignored severe hypoglycemia can occur which may be dangerous and difficult to treat [15]. Post-exercise and late onset hypoglycemia: Post-exercise hypoglycemia and late onset hypoglycemia (LOH) can occur up to four and 24 hours after exercise respectively [1,24]. The incidence of LOH might be increased in wellcontrolled diabetic subjects; because, these patients may have high insulin levels and normal or near normal blood glucose before exercise [24]. Hypoglycemia after exercise may be consequences of refilling the glycogen stores which are depleted in exercise and/or increase the tissue sensitivity to insulin [12,15]. Usually, after several days of exercise training, the need to insulin gradually decreases [15]. Nocturnal hypoglycemia may disturb sleep patterns, alter recovery, and therefore affect physical performance in the following day and also it may cause severe morbidity and even mortality. Consuming an evening snack or reduction of evening dose of insulin after activity may be useful in this situation [1]. Little information is available for nutritional adjustment to prevent LOH [24]. Treatment of exercise induced hypoglycemia: If hypoglycemia occurs, the patient should stop physical activity and monitor his blood glucose level every 15 minutes until it is higher than 80 mg/dL. The patient should take a rapid-acting carbohydrate (3-4 glucose tablets [4 g each] or a half cup of apple or orange juice). If hypoglycemia persists, additional carbohydrate may be needed. The patient could return to his activity when he or she feels better and blood glucose level are >100 mg/dL [2,12,20]. After exercise, blood glucose should be checked and if intensity and duration of exercise is high a recheck is needed to avoid late onset of hypoglycemia [16]. A rapidly absorbed carbohydrate in the form of simple sugar (e.g., fruit juice, hard candy) must be available during the activity [2,20]. It is important to determine the causes of hypoglycemia, it may be due to a high daily dose of insulin and insufficient reduction of insulin, errors in insulin dosage, insufficient or delayed food intake, alcohol intake during or immediately after exercise [2]. Hyperglycemia Exercise could cause hyperglycemia in the subjects with IDDM. Hyperglycemia cold happen in three situations; first, when the subjects are metabolically unstable and the level of insulin is very low [15]; second, during a short high intensity exercise [2]; and third, as a result of over consumption of food[19]. During exercise, when the level of blood insulin is very low, hepatic glucose production increases and glucose uptake by the muscles decreases. On the other hand, secretion of the counter-regulatory hormones such as catecholamines, glucagon, growth hormone and cortisol is increased which could cause hyperglycemia [15]. As a result when the level of insulin is low exercise is contraindicated [7]. Exercise in this situation could lead to ketosis, increase lactate, osmotic symptoms of hyperglycemia, fatigue, muscle cramps and poor athletic performance [15]. During a very high intensity short duration exercise such as weight lifting blood glucose can increase due to a significant increase in catecholamine secretion. It is usually transient, and blood glucose level usually decreases for several hours after exercise [2,15]. Hyperglycemia after exercise is often due to over-intake of food before and during exercise which may be due to fear of hypoglycemia [15, 19]. Feet Health Foot problems are the main cause of hospitalization of people with diabetes. About 15% of diabetics have a foot or leg ulcer [2]. Proper footwear is essential and also the use of silica gel or air midsoles and polyester or blend (cotton-polyester) socks to prevent blisters and keeping the feet dry is important for minimizing trauma to the feet [7]. Diabetics should carefully evaluate their feet for blisters and other potential injuries, both before and after physical activity [7]. Neuropathy is not a contraindication for exercise, but, special attention for soft tissue, bone and joint injuries is needed. Stretching muscles before exercise is important to prevent ligament strain. Swimming or bicycling is the recommended forms of exercise for these patients [8, 25]. Hydration Appropriate hydration is also essential in diabetic athletes, as dehydration can affect blood glucose level. Diabetic athletes should use adequate fluid before, during and after exercise and sports, especially during hot and humid weather. Recommendations for fluid intake in diabetics are the same as non-diabetics athletes [7, 19]. Environment In a hot weather, the rate of insulin absorption may increase due to vasodilatation and increase the blood flow in the skin. Therefore the risk of hypoglycemia is higher when exercising in hot and humid conditions [15]. Also, in cold weather fuel consumption is increased because of shivering and increased resting metabolic rate. Therefore cold weather can also increase the risk of hypoglycemia [7, 15]. Conclusion The number of diabetic athletes is increasing in the world [3]. But it is suggested that there are not enough documents in this field [4]. Type 1 diabetic subjects without any complications and with a good blood sugar control can engage in all levels of sports activities, both recreational and professional [7]. A detail pre-participation physical examination is needed to find out if there are any complications [12]. All diabetics should be encouraged in performing suitable exercise and sports. The recommended physical activities are moderate aerobic activities [7, 8]. To prevent acute diabetic side effects of exercise, diabetic athletes should have an adequate control of blood sugar before starting exercise. Also, nutrition and insulin dosage may require some adjustment. Depending on the type of exercise, ambient environment and the level of blood glucose before exercise, diabetic athletes need to consume some carbohydrate before, during and may after exercise. If the exercise takes more than 30 minutes the insulin dose should be decreased by 14-50% [15, 19]. Every athlete should find his or her own approach in the management of nutrition and insulin adjustment and integrity of them with exercise and sport. This could be achieved by trial and error using basic scientific recommendation. Special attention should be provided for foot problems especially for the cases with long standing diabetes. More research is needed in the variety of aspects of exercise and sports in type 1 diabetes; such as the effects of different kinds of sports on diabetes, the effects of exercise and sports on subgroups of patients such as adolescents and kids and the prevention of late onset hypoglycemia. References
Copyright 2007 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe07010t3.jpg] [pe07010t2.jpg] [pe07010t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}