 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
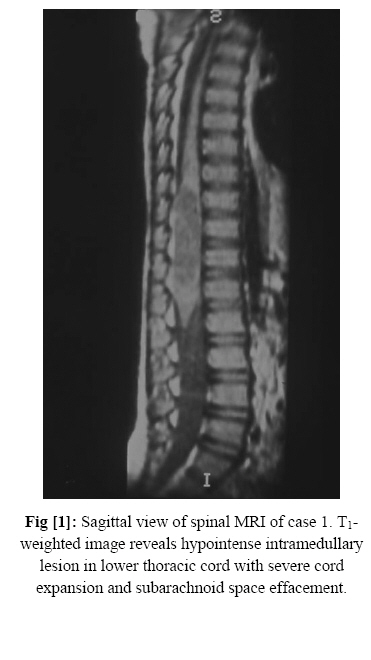
Intramedullary Spinal Cord Abscess: Report of Two Cases Farideh Nejat* 1, MD; Ghamar Taj Khotaei 2, MD; Setareh Mamishi 2, MD 1Department of Neurosurgery, Tehran University of Medical Sciences, IR Iran 2, Department of Pediatrics, Tehran University of Medical Sciences, IR Iran Received: 16/9/06; Code Number: pe07012 Abstract Background: Intramedullary spinal cord abscess is a treatable cause
of paraparesis. It can
rapidly lead to complete paralysis below the lesion. Key Words: Abscess, Antibiotics, Child, Spinal cord, Laminotomy Introduction Intra-medullary abscess is extremely rare [1]. Fewer than 100 cases have been reported since this condition was first described by Hart in 1830[2,3]. It may be confused with transverse myelitis or Guillian-Barre syndrome or may be thought to be intramedullary tumor in a more chronic disease. Commonly it arises by hematogenous spread from distant foci of infection. The thoracic spinal cord is most often involved. Frequently no known antecedent infection can be identified [1]. In this article we report two cases of spinal cord abscess in pediatric age group. Cases Presentation Case 1: A 3-year-old boy was admitted with a history of progressive paraparesis since 2 months ago. There was a history of diarrhea and then band like abdominal pain several weeks before beginning of his neurological deficits that had been evaluated for abdominal pain. He had severe paraparesis, urinary incontinence and sensory level up to xyphoid. There wasn't any skin abnormality on his back. Spinal magnetic resonance imaging (MRI) revealed an intramedullary lesion from 10th thoracic to the first lumbar spinal level (T10-L1). It was nonhomogen, hypointense to isointense on T1weighted image and hyperintense on T2weighted image (Fig 1). The diagnosis of an intramedullary tumor was thought to be the first. Osteoplastic laminotomy from T10 to L1 was done to remove the mass. There was adhesion between pia mater and dura mater, cord was very tense. Dorsal myelotomy at the upper portion yielded yellowish purulent fluid, so myelotomy stopped and about 10cc pus removed. After drainage and irrigation of the cavity, cord was completely decompressed. We didn't find any true capsule for the cavity, so biopsy was not done. Culture of the sample was positive for E. coli. Antibiotic therapy continued for 6 weeks. He found some sensory recovery and return of leg movement. Still after 3 years, he isn't able to walk on his own, his sphincter problem is persistent and managed with clean intermittent catheterization. Follow-up MRI one year after surgery was free of disease. Case 2: A 4-year-old male was admitted due to complaints of left leg paresis, frequency and urge incontinence. The child had paraparesis, left leg was weaker than right, but he could stand and walk without any help. There wasn't any history of febrile disease and abnormal laboratory tests. MRI demonstrated cystic intramedullary mass from 9th thoracic to the first lumbar spinal level (T11-L2), hypointense on T1-weighted image and hyperintense on T2-weighted image, without enhancement with Gadolinium injection (Fig 2). We considered the diagnosis of an intramedullary cystic lesion, most probably abscess or dermoid tumor. Osteoplastic laminotomy at T12 level was done and with aspiration of intramedullary cyst 8cc pus removed to decompress the cord. There wasn't any capsule for abscess. The smear showed many polymorph nuclear cells and gram-positive bacteria, but negative culture. He was treated with ceftriaxone, vancomycin and metronidazole for 6 weeks. He found good recovery of neurological deficits early after decompression surgery. At the time of discharge, his sphincter problem had surprisingly been improved completely. Now after 2 years, he is free of disease, with normal neurological exam and normal MRI. Discussion Intramedullary spinal cord abscess is extremely rare [4]. This occurs much more rarely than brain abscess. The reduced volume of spinal cord tissue probably accounts for the relative rarity of spinal abscess[5]. It is described only in case reports. The presentation can be very confusing and mimic thoracic or abdominal diseases [6]. Acute cases evolve in a few days as a transverse myelitis, subacute and chronic cases mimic an intramedullary tumor of the posterior cord [5]. Some patients may complain of pain, most experience only progressive spinal cord dysfunction. Many patients, even those presenting acutely may be afebrile[2]. The peak incidence occurs in the first and third decades, males are more commonly affected than females, about 25 percent of cases occur in children aged younger than 5 years [4]. Thoracic cord is affected in 80 percent of the patients. The cervical spinal cord was least likely to be affected [5]. Intramedullary abscesses are most common in immunecompromised patients including the HIV infected and IV drug abusers [1,4]. Antecedent infections of the respiratory tract, spine, heart valves, genitourinary tract and soft tissues and midline spinal skin defect such as dermoid sinus maybe found. About 80 percent of abscesses are solitary [4]. The peripheral blood leukocyte count may be elevated. Cerebrospinal fluid [CSF] may have increased cells and protein or be normal. CSF cultures are almost always negative[2]. The erythrocyte sedimentation rate [ESR] tends to be elevated regardless of their clinical findings[7]. Plain X-ray is usually negative. MRI is the choice diagnostic test. MRI reveals involvement of over two cord segments[2], abscesses are hypointense on T1- and hyperintense on T2weighted image, contrast enhanced MRI can demonstrate nodular area of enhancement or ring enhancement on T1-weighted images[8,9]. Our patients` MRI had shown the same intensity changes as mentioned above with near four segments involvement, but without enhancement in case 2. Staphylococcus and Streptococcus are the most common identified organisms (23.7% and 17.2% respectively), whereas most cultures (38.7%) remain sterile [2]. Bacteria reach the spinal cord via direct implantation, lymphatic or hematogenous spread. Hematogenous spread is the most common way [4]. The primary source of infection could be found in only 45% of patients[7]. Prompt surgical drainage accompanied by antibiotics is the optimal treatment [2,10]. Laminectomy is performed at the appropriate level followed by aspiration of the cord at its widest point. Surgical aspiration should be performed as an emergency measure. Limited laminotomy is the choice treatment in children and prevent postoperative kyphosis. Occasionally an intramedullary abscess masquerades as arachnoiditis and therefore when localized, spinal arachnoiditis is discovered during operation on the spinal cord, the surgeon must ensure that a cord abscess is not missed. Duration of antibiotic therapy has not been established, it is related to organism, patient and the course of response. Biopsy from the abscess cavity was not possible in both cases due to lack of obvious wall. Postoperatively patients should be closely followed for an extended period because of the high recurrence rate. Up to 25 percent of patients require redrainage [2]. In the past patients who did not undergo surgical drainage of abscesses usually died. Therapeutic success depends largely on prompt diagnosis and effective drainage. Appropriate antibiotic therapy after surgical drainage is warranted. If left untreated, the outcome is bleak. Motor and sphincter function seem to find best recovery, but sensory loss less well. There is good improvement in 66 percent of patients [2]. Our first case could not find acceptable recovery due to delayed diagnosis and severe neurological deficits on admission. The second case, which was treated at earlier phase of disease, found complete recovery. Conclusion Although intramedullary spinal cord abscess is a rare disease, we should have knowledge of its existence because misjudgment and deferring adequate treatment may lead to an unfavorable outcome. In these patients, a lesional biopsy is not needed to make the diagnosis; biopsy of the lesion uniformly exacerbates the condition and should be avoided. References
Copyright 2007 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe07012f2.jpg] [pe07012f1.jpg] |
| |||||||||

{kind=link}
{kind=link}