 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 17, No.4, December 2007, pp. 339-344 The Effect of Kangaroo Care on Physiologic Responses to Pain of an Intramuscular Injection in Neonates Firoozeh Sajedi*1, MD; Zahra Kashaninia2, MSN; Mehdi Rahgozar3, PhD;Fariba Asadi Noghabi4, MSN 1Pediatrician, Department of Clinical Sciences, University of Welfare & Rehabilitation, Tehran, IR Iran Received: 13/4/07; Revised: 19/9/07; Accepted: 31/10/07 Code Number: pe07064 Abstract Objective: Pain in neonates can be associated with various risks. So, it seems essential to find a
simple and acceptable method for relieving pain. Pharmacologic agents are not recommended in
neonates for pain relief in minor procedures but nonpharmacologic interventions like Kangaroo Care
(KC) is found to be effective. The objective of this study was to assess the efficacy of KC on
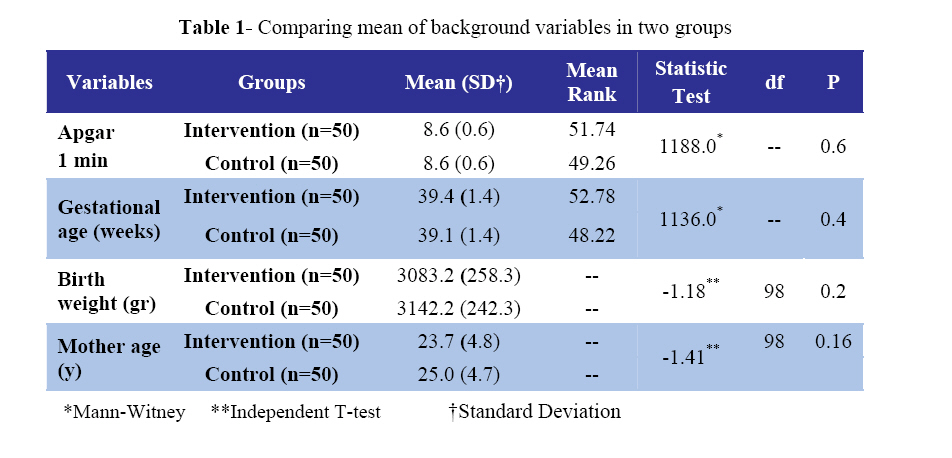
physiologic responses to the pain of an intramuscular injection of vitamin K in term neonates. Key Words: Term neonates, Intramuscular injection, Kangaroo Care, Physiologic responses, Pain Introduction The deleterious effects of pain in infants are fairly well described. They include physiologic and metabolic effects such as vital sings changes, alteration in cerebral blood flow, and outpouring of stress hormones.[1] With pain, an increase in the activation of sympathetic nerve fibers innervating the heart causes the sinoatrial node to produce an increase in the heart rate (HR). Heart rate is low during restful situations and sleep, and becomes elevated during periods of activity, stress, and pain [2,3], the magnitude of the HR change is related to the intensity and duration of the stimulus [4], and to individual temperaments of the infants[5]. Nonetheless, with heel stick, HR generally increases 18 beats per minute (bpm) in 27 weeks postmenstrual age infants [6] and 9 bpm in 27 to 35 weeks postmenstrual age (PMA) preterm infants. HR rose 12 and 36 bpm in term infants [7,8] in response to heel stick. If infants cry and become agitated with pain, HR increases further. Oxygen saturation decreases in response to pain.[9,10,11,12] During episodes of vigorous crying, oxygenation may increase but oxygen delivery to cerebral tissues may be compromised even though the oxygen content of the blood remains stable.[11] Preterm infants are usually maintained at or returned to oxygen saturations that are either low (88% to 90%), standard (91% to 95%), or high (95% to 98%).[13] However, with pain, oxygen saturation drops commonly 3% to 4% below the infant’s baseline for the duration of the painful procedure, and may even drop below 88% for sustained periods if analgesics are not given.[10,14] It is important to anticipate painful experiences while child is hospitalized or receiving medical treatment. Most acute pain experiences in medical settings can be prevented or substantially relieved.[15] The American academy of pediatrics, in conjunction with the Canadian paediatric society, and the American pain society developed policy statement addressing the need to minimize painful or stressful procedures and eliminate pain-associated suffering.[15,16] Kangaroo Care (KC) may be an effective method to blunt pain responses because some of its components have been found to reduce the severity of responses to stress. For example, containment acts to prevent an increase in behavioral distress and plasma cortisol after a heel stick [17], and the presence of maternal heart beat, a sound can be perceived by the infant as he/she lies against the maternal chest, prevents full-term newborns from significantly increasing serum and salivary cortisol levels after painful stimulation.[18] The vestibular component of carrying, similar to the gentle stimulation of the mother’s chest respiratory movements, produces a comforting effect during painful stimulation[19]. Being in a calm and comforted state is suggested by autonomic stability observed during KC.[20,21,22] Thus, an experimental study was conducted to measure the effect of KC on physiologic (heart rate and oxygen saturation) measures of pain before, during, and after an intramuscular injection of vitamin K. Material & MethodsFollowing approval by the Ethics Committee of the University of Welfare and Rehabilitation Sciences and informed consent from the parents, data were collected from 100 healthy newborns delivered at Shariati hospital in Bandar Abbas City (Iran). Inclusion criteria were birth weight between 2500 and 4000 grams, age of birth 2 to 24 hours, Apgar Scores of at least 7 at 1 minute, estimated gestational age of at least 37 weeks, heart rate between 100 and 160 per minute, blood 02 saturation ≥95% and no known congenital anomalies. Exclusion criteria were caesarean section, administration of a vaccination or any injection, birth trauma, ill neonate and drug abuse by the mother in pregnancy. The neonates were randomly assigned to intervention and control groups. The number of samples in each group was 50. Demographic characteristics were essentially homogenous between the 2 groups (Table 1). Mean birth weight was 3083.2 grams (SD= 258.3) and 3142.2 (SD=242.3) in intervention and control groups respectively. Data were collected in a quiet room in the nursery. The infants were brought to a quiet, alert state at the start of data collection. Control infants were wrapped in their receiving blanket and placed on their side in their respective bassinets. Mothers, whose infants had been assigned to receive contact, changed into a hospital gown that buttoned in front and returned to their beds that had been adjusted to a 45° angle to provide a comfortable reclining position. Then the infant, wearing only a diaper, was then positioned on the mother so that skin-to-skin contact was maintained through her open gown. Two receiving blankets were placed over the infant’s back. The mothers then were asked to lock their fingers, place their hands over the blankets, and apply a slight pressure on their infant’s back to stabilize the infant for both procedural ease and to facilitate video recording. The mothers were requested not to rub their infant’s head, speak with their neonates, shake them, or touch them before, during, or after the injection. At this point, the experimenters left the room for 10 minutes, so that mother and infant could settle into a relaxed contact position. On return, we found infants in both groups to be in a relaxed and quiet state. So the sequence of phases was as follows:
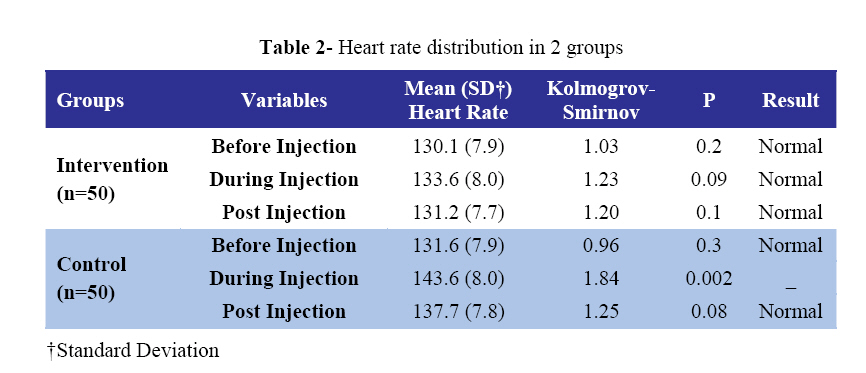
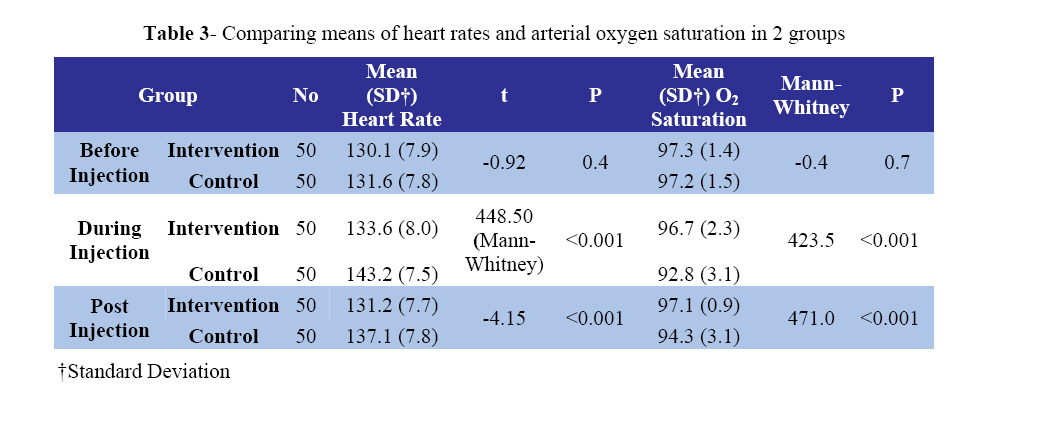
Data were analyzed using SPSS for Windows. Independent-t, Mann-Whitney and Chi-square tests were used for analysis. Kolmogrov-Smirnov test was used to check normality of distributions. FindingsOne-hundred neonates were randomized during a 2-month observation period; similar demographic characteristics were demonstrated between the two groups (Table 1). Number of females in the intervention and control group was 28 (56%). The heart rate distribution before, during and after injection was normal in 2 groups (Table 2). There was no significant difference in mean heart rate before injection (P=0.4), but during (P<0.001), and after (P<0.001) injection between the 2 groups (Table 3). There was no significant difference in the blood oxygen saturation before (P=0.7), but during (P<0.001), and after (P<0.001) injection between the 2 groups (Table 3). Discussion In this work we assessed the efficacy of KC physiologic responses to the pain of an intramuscular injection of vitamin K in healthy term neonates. Based on the results of this study, there were significant differences in the mean heart rate and blood oxygen saturation after minor painful procedure between the KC group and control group. So we demonstrated that KC given before intramuscular injection attenuated the increase in the heart rate and the decrease in blood oxygen saturation which are associated with minor painful procedures. It is of therapeutic relevance to study pain therapy for minor painful procedures that are performed frequently during neonatal care especially intensive care. Neonates are more sensitive to cutaneous stimuli than adults [24] and repeated skin punctures affect their subsequent pain perception [25] and their behavioral and autonomic pain reactions.[26] Though this study was not designed to address mechanisms contributing to a reduction in pain response, 2 other studies, each using the same methodology but differing in their outcomes, provide a possible explanation. Mooncey [27] as well as Modi and Glover’s [28] studies indicated that pain responses may be diminished due to KC's ability to deactivate the hypothalamo- pituitary-adrenal axis (HPA) and may consequently alter pain responses. KC has been suggested by some to be a form of touch that promotes the infant's ability to moderate the effects of painful factors because KC increases opioid peptide secretion.[29,30] In animals, nonnoxious stimulation, such as stroking, skin-toskin contact, massage, and pleasant warm temperature, causes a release in oxytocin that enhances the antinociceptive effects of these treatments.[31] The clinical usefulness of 15 minutes of KC needs to be addressed in future studies too, given that only 20 minutes of KC has been effective in deactivating the HPA axis[28] and 30 minutes of KC has been shown to reduce facial grimacing and Premature Infant Pain Profile scores.[32] Gray et al [8] conducted a randomized controlled trial that compared healthy term neonates, 15 of whom were given KC for 10 to 15 minutes before heel stick and remained in KC for the heel stick, to 15 who were swaddled in their crib during a heel stick for routine blood sampling. Heart rate, crying time, and facial grimacing were recorded for a 2-minute baseline, throughout the 155 to 159 second blood draw, and for a 3-minute recovery period. Crying was reduced by 82%, grimacing by 64%, and heart rate increased 8 to 10 bpm in the KC group as compared to 36 to 38 bpm in the swaddled group. Gray [23] followed with a similar study evaluating the full-term infant’s pain response when heel stick was conducted as the infant lay in KC during breast feeding. HR rose 6 beats per minute during KC heel stick and 29 beats per minute during cot heel stick. Repeated use of KC to modify infant pain raises the question of the possibility that an infant may make associations between KC and a painful experience. Animal studies suggest that simultaneous close contact and sucking prevent activation of afferent pathways to the brain, preventing cortical activation and, thus, associative memory.[33] Also, this concern has not been substantiated in studies of older children being held by their mothers for surgical procedures.[34] precautions taken to prevent the association in older children, such as long periods of maternal-child contact prior to the painful procedure and intensification of maternal-infant contact by holding the infant more firmly and adding soothing vocalizations and stroking after the procedure, may be useful with premature infants, too. Premature infant's tolerance of simultaneous multisensory input with scrutiny for signs of physiologic compromise will need to be established. Given that nurses have positive attitudes about relieving pain and use behavioral interventions to do so [35], the results reported here will support KC's implementation for procedural pain. Conclusion This study adds one more piece of evidence that pain responses, measured physiologically, are significantly reduced in neonates undergoing intramuscular injection when they are given 10 minutes of KC before the injection and have the injection performed in KC. Kangaroo care is a nonpharmacologic intervention to manage neonate procedural pain that can be implemented without concern for physiologic compromise in neonates. Acknowledgment We would like to thank Chancellor and Vice-Chancellor for research of The University of Social Welfare & Rehabilitation Sciences for their ongoing financial support. We would also like to acknowledge the parents of neonates and staff of Shariati Hospital of Bandar Abbas for their cooperation. References
Copyright 2007 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe07064t3.jpg] [pe07064t2.jpg] [pe07064t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}