
|
Iranian Journal of Pediatrics
Tehran University of Medical Sciences Press
ISSN: 1018-4406 EISSN: 2008-2150
Vol. 17, Num. 4, 2007, pp. 353-358
|
Iranian Journal of Pediatrics, Vol. 17, No.4, December 2007, pp. 353-358
Prevalence and Symptoms of Idiopathic Hypercalciuria in Primary School Children of Tehran
Seyed Taher Esfahani1, MD; Abbas Madani1, MD; Ali Ashraf Siadati1, MD;
Mohammad Nabavi2MD
1Department of Pediatric Nephrology, Tehran University of Medical Sciences, IR Iran
2Department of Pediatrics, Semanan University of Medical sciences, Iran
* Correspondence author; Address: Pediatrics Nephrology Ward, Children’s Medical Center, Dr Gharib Ave, Tehran, IR Iran E-mail: esfahani@sina.tums.ac.ir
Received: 12/04/07; Revised: 04/08/07; Accepted: 03/10/07
Code Number: pe07066
Abstract
Objective: Determining prevalence of idiopathic hypercalciuria (IH) in primary school children of
Tehran.
Material & Methods: We evaluated 778 primary school children (age 6-11, mean 9.1 years) in two
steps: first (Screening test), we measured urine calcium to urine creatinine ratio (UCa/UCr) and in the
second step (Definitive test), for those children who had UCa/UCr ratio more than 0.21 mg/mg we
measured 24 hours urine calcium excretion. Children with secondary forms of hypercalciuria were
excluded from the study. Children with idiopathic hypercalciuria were evaluated for manifestations of
IH.
Findings: Among 778 children, 195 (25.1%) had UCa/UCr ratio more than 0.21 mg/mg, but from
these 195 children only 128 children delivered 24 hours urine samples. Among these 128 children for
whom 24 hours urine calcium measurements were done 28 children excreted more than 4mg/kg/day
calcium without hypercalcemia or any other known causes of hypercalciuria and we defined them as
having idiopathic hypercalciuria. If all 195 suspicious cases of IH had delivered 24-hrs urine samples
we would have 42 cases of IH.
Conclusion: Prevalence of IH in our children was 5.4% and its manifestations were: hematuria,
dysuria, recurrent abdominal pain, urinary incontinence, urgency, urinary tract infections and
urolithiasis.
Key Words: Idiopathic hypercalciuria, Children, Urolithiasis, Hematuria, Dysuria, Urgency
Introduction
Idiopathic hypercalciuria (IH) is one of the most
common human metabolic abnormalities and is
present in approximately 60% of individuals with nephrolithiasis.[1] Anecdotal and uncontrolled
data point to association between IH and signs
and symptoms like hematuria, development of
calcium oxalate nephrolithiasis, dysuria, urinary frequency, enuresis, abdominal and back pain, and urinary tract infection.[2-4] There is a worldwide variation in prevalence of IH in children from 0.6% in Japan[5] to 26% in France[6]. Because there is not a report regarding prevalence of IH in Iranian children, we studied the prevalence and symptoms of IH in a large group of healthy primary school children living in Tehran.
Material & Methods
This is a descriptive and cross-sectional study. From October 1999 to February 2000, we went to some of primary schools in Tehran and with informed consent of parents, school directors and teachers we collected non-fasting random urine specimens from children. At this stage only healthy children were included into the study. After determining urine concentration of calcium and creatinine, children whose urine calcium to urine creatinine (UCa/UCr) ratio was more than 0.21 mg/mg, were defined as suspicious cases of hypercalciuria. 24 hours urine specimens were collected from these children and urine calcium excretions were measured. Children whose 24 hours urine calcium excretion exceeded 4 mg/kg body weight were defined as hypercalciuric children. In hypercalciuric children we performed physical examinations and laboratory tests (serum calcium, phosphorus, alkaline phosphates, PTH, urinalysis, urine culture, and 24 hours urinary protein). Children with secondary forms of hypercalciuria were excluded from the study.
Urine calcium was measured by colorimetric method with methylthymol blue. The 8-hydroxyquinolon was used to prevent Mg2+ ions interfering. Urine creatinine was measured by kinetic Jaffe reaction. All measurements were done by Automatic Analyzer, HITACHI 704 Boehringer Manheim.
Descriptive statistics included mean and standard deviation (SD) used for UCa/UCr ratios and 24 hour urine calcium excretion parameters. This study was approved by the Research and Ethics Committee of Tehran University of Medical Sciences.
Findings
Seven hundred and seventy eight primary school children aged 6-11 years (mean 9.1 years) were recruited into the study. Four-hundred seventy one of children (60.5%) were boys and 307 (39.5%) were girls. At this stage 195 children (25.1%) had UCa/UCr more than 0.21 mg/mg, 143 (73.3%) of them were boys and 52 (26.7%) girls. Of 195 children who had hypercalciuria, only 128 children delivered 24 hours urine samples.
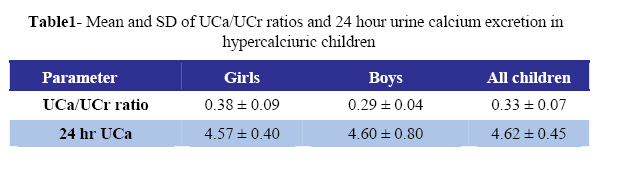
Among these 128 children of whom 24 hours urine calcium measurements were available, 28 children (21.9%) excreted more than 4mg/kg/day calcium without hypercalcemia or any other known causes of hypercalciuria and we defined them as having idiopathic hypercalciuria. So if all 195 suspicious cases of IH had delivered 24-hrs urine samples we would have 42 cases of IH. Thus, prevalence of IH in our children is 5.4%. Among these children 16 (57.2%) were boys and 12 (42.4%) girls. Mean (SD) of UCa/UCr ratio and 24 hours urine calcium of these children are shown in table 1.
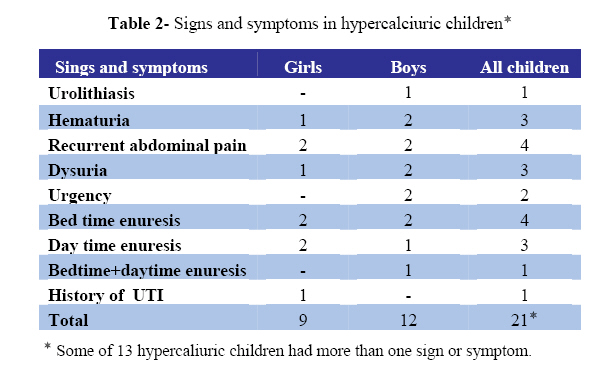
Seven of these 28 children had familial history of urolithiasis and 13 of them had signs or symptoms which could be due to IH (Table 2).
Discussion
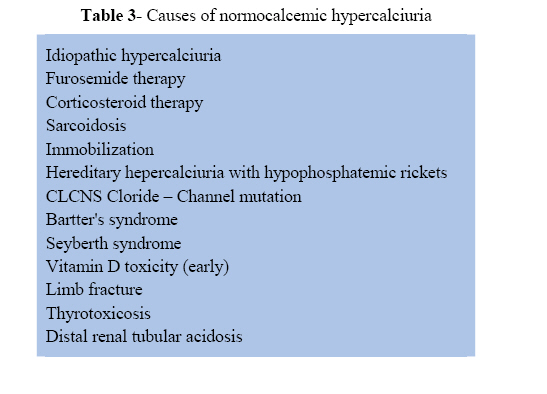
Hypercalciuria is named idiopathic if serum calcium level is normal and known causes of normocalcemic hypercalciuria (table 3) can be excluded.[7] IH is a common metabolic abnormality in children. The precise definition of idiopathic hypercalciuria has not been yet established, but in current clinical practice, the upper limit of normal for calcium excretion in children is generally considered to be 4 mg/kg/day.[8] Urinary calcium is best measured in 24-h collection. However such collections are difficult to obtain in children and many investigators have used the urinary calcium/ creatinine ratio (UCa/UCr) as alternate measurement.[7-12] As in our study, some authors have used UCa/UCr ratio as a screening test and 24-h urine calcium as definitive test of diagnosing hypercalciuria.[7,13] Hypercalciuria is likely present when a randomly voided urine sample shows a calcium to creatinine ratio (both values in milligrams) exceeding 0.21.[7,8]
There is a wide variation in prevalence of IH in different countries. The lowest prevalence is reported from Japan: 0.6%.[5] Reported prevalence in other countries has been Germany 8.6%[14], Italy 9.1%[15], USA 12-13%[16 ,17], Turkey: 2.9%[18], Argentina 12.7% [19], and France 26%.[6] In our study it was 5.4%.
Most cases of IH are asymptomatic. The prevalence of symptoms and signs in children is different in reported surveys. In our study 46.4% children were symptomatic. Because the number of children is low, determining prevalence of each symptom is not possible.
IH is a complex disease resulting from an inheritance and is compatible with autosomal dominant transmission.[20-22] Many candidate genes have bean studied to determine their role in the pathogenesis of hypercalciuria, but most of the candidate genes have produced negative to only marginal results[20, 23-27]. It seems that we are still on the way to discovering genes with a role in IH[26]. It is probably the most commonly diagnosed metabolic disorder in adults with renal calculi.[1,7,22,28,29] Between 30-50% of calcium stone formers have idiopathic hypercalciuria.[30] In a reported from UK, IH was defended in 25% of children with calculi.[31] The risk of nephro- lithiasis increases progressively with the greater levels of IH.[29] In 85% of children with IH, renal calyceal microlithiasis has been reported in follow up sonographies.[32]
Children with IH have been noted with increasing frequency to manifest an array of predominantly lower urinary tract signs and symptoms, these symptoms and signs are probably due to micro crystallization with injury to the urinary tract epithelia.[33]
Microscopic hematuria, urinary frequencyurgency syndrome, daytime incontinence, colicky abdominal pain, recurrent urinary tract infections and episodic gross hamaturia are the most common clinical symptoms in children with IH.[7, 33,34]. Hematuria is the major noncalculi manifestation of IH in children.[28,35-37] The presence of hematuria in a child with IH also appears to be a strong predictor for the subsequent development of calcium oxalate nephrolithiasis.[37] Microscopic hematuria due to IH is asymptomatic; whereas some discomfort such as dysuria or suprapubic pain is often seen with gross hematuria. The gross hematuria is often transient, although a few children have been reported to have gross hematuria lasting for several days.[36,37]
IH can produce dysuria-urinary frequency in children [2,33] and irritability in infants.[3] Also in a study of 124 children with idiopathic hypercalciuria 28 (23%) had urinary incontinence.[38] IH may have a significant role in cases of functional voiding disorders.[39] IH also has been implicated in producing nocturia in some children.[7] Uncontrolled data also point to a possible association between IH and some cases of enuresis.[7]
Recurrent abdominal and flank pain is also reported in children with IH.[40,41] IH may be a contributing factor to recurrent UTI in children.[42]
In recent years a great deal of attention has been directed towards the potential effect of IH on bone mineral density. Reduction of bone mineral density has been reported in both children [43-46] and adults [47-50] with IH.
IH had been traditionally divided into absorptive and renal types. This classification has been debated intensely in the literature. The current view is that both types are continuum and can occur in a child with IH [51,52]. So in our study we did not try to characterize type of IH in children.
Conclusion
Prevalence of IH in our children was 5.4% and its manifestations were: hematuria, dysuria, recurrent abdominal pain, incontinence, urgency, urinary tract infections and urolithiasis.
References
- Levy FL, Adams–Huet B, Pak CY. Ambulatory evaluation of nephropithiasis: an update of a 1980 protocol, Am J Med. 1995; 98(1):50-59.
- Alon US, Warady BA, Hellerstein S. Hypercalciuria in the frequency–dysuria syndrome of childhood, J Pediatr. 1990; 116(1):103-5.
- Fivush B. Irritability and dysuria in infants with idiopathic hypercalciuria, Pdiatr Nephrol. 1990;4(3):262-3.
- Lopez MM, Castillo LA, Chavez B, et al. Hypercalciuria and recurrent urinary tract infection in Venezuelan children. Pediatr Nephrol. 1999;13(5):433-7.
- Kaneko K, Tsuchiya K, Kawamura R, et al. Low prevalence of hyperclciuria in Japanese children. Nephron, 2002;91(3):439-43.
- Royer P, Habib R, Mathieu H. Nephrologie im Kindesalter. Stuttgart; Thiwme. 1967.
- Langman CB. Disorders of phosphorus, calcium and vitamin D. In: Avener ED, Harmon WE, Niaudet P (ed). Pediatric Nephrology. 5th ed. Philadelphia; Lippincott, Williams and Wilkins. 2004; Pp:237-54.
- Butani L, Kalia A. Idiopathic Hypercalciuria in children, how valid is the existing diagnostic criteria? Pediatr Nephrol. 2004; 19(6):577-82.
- Ring E, Brokenstien M: Use of calcium creatinine ratio in diagnosis and therapy, Padiatr Padol. 1987;22(3):245-50.
- Hingelfeld MS, Simon S, Blowey D, et al: Lack of seasonal variation in urinary calcium / creatinine ratio in school-age children. Pediatr Nephrol. 2004;19(10):1153-5.
- Alon US, Berenbom A. Idiopathic hypercalciuria of childhood, 4 to 11-years outcome. Pediatr Nephrol. 2000;14(10-11):1011-5.
- Tekin N, Kural N, Tourn M: Renal function in children with hypercalciuria. Turk J Pediatr. 1997;39(3):335-9.
- So NP, Osorio AV, Simon SD, et al. Normal urinary calcium/creatinine ratios in African-American and Caucasian children, Pediatr Nephrol. 2001;16(2):133-39.
- Manz F, Kehrt R, Lausen B, et al. Urinary calcium excretion in healthy children and adolescents. Pediatr Nephrol. 1999;13(9): 894-9.
- De Santo NG, Di Iorio B, Capasso G, et al: Population based data on urinary excretion of calcium, magnesium, oxalate, phosphate and uric acid from Cimitile (southern Italy). Pediatr Nephrol. 1992;6(2):149-57.
- Welch TR, Abrams SA, Shoemaker L, et al. Precise determination of the absorptive component of urinary calcium excretion using stable isotopes. Pediatr Nephrol. 1995;9(3): 295-7.
- O'Brien KO, AbramsSA, Stuff JE, et al. Variable related to urinary calcium excretion in young girls. J Pediatr Gastoenterol Nutr, 1996;23(1):8-12.
- Bercem G, Cevit O, Toksoy HB, et al. Asymptomatic hypercalciuria: Prevalence and metabolic characteristics. Indian J Pedaitr. 2001;68(4):315-8.
- Alconcher LF, Castro C, Quintana A, et al. Urinary calcium excretion in healthy school children. Pediatr Nephrol. 1997;11(2):186-8.
- Nicolaidou P, Themeli S, Karpathios T, et al. Family pattern of idiopathic hypercalciuria and its subtypes. J Urol. 1996;155(3):1042-4.
- Coe FL, Parks JH, Moore ES. Familial idiopathic hypercalciuria. N Engl J Med. 1979;300(7):337-40.
- Scheinman SJ. Nephrolithiasis. Semin Nehprol. 1999;19(4):381-8.
- Soylemezoglu O, Ozkaya O, Gonen S, et al. Vitamin D gene polymorphism in hypercalciuric children. Pediatr Nephrol. 2004;19(7):724-7.
- Vezzoli G, Tanini A, Ferrucci L, et al. Influence of calcium-sensing receptor gene on urinary calcium excretion in stone–forming patients. J Am Soc Nephrol. 2002;13(10): 2517-23.
- Muller D, Hoenderop JG, Vennekens R, et al. Epithelial Ca2+ channel (ECAC1) in autosomal dominant idiopathic hypercalciuria. Nephrol Dial Transplant. 2002;17(9):1614-20.
- Gambaro G, Vezzoli G, Casari G, et al. Genetics of hypercalciuria and calcium nephrolithiasis; from rare monogenic to common polygenic forms. Am J Kidney Dis. 2004;44(6): 963-86.
- Petrucci M, Scott P, Quimet D, et al. Evaluation of the calcium-sensing receptor gene in idiopathic hypercalciuria and calcium nepholithiasis. Kidney Int. 2000;58(1):38-42.
- Escribano SJ, Rodriguez MV Rovira AF, et al. Idiopathic hypercalciuria: clinical manifestation and risk for urolithiasis in children. An Esp Pediatr. 1997;46(2):161-6.
- Lerolle N, Lantz B, Paillard F, et al. Risk factors for nephrolithiasis in patients with familial idiopathic hypercalciuria. Am J Med. 2002;113(2):99-103.
- Coe FL, Favus MJ, Asplin JR. Nephrolithiasis in Brenner BM (ed): Brenner and Rector's: The Kidney, 7th ed. Philadelphia, Saunders. 2004; Pp:1819-65.
- Coward RJM, Peters CJ, Duffy PG, et al. Epidemiology of pediatric renal stone disease in the UK. Arch Dis Child. 2003;88(11):962-5.
- Escribano J, Balaguer A, Martin R, et al. Childhood idiopathic hypercalciuria – clinical significance of renal calyceal microlithiasis and risk of calcium stones. Scand J Urol Nephrol. 2004;38(5):422-6.
- Heiliczer JD, Canonigo BB, Bishof NA, et al. Noncalculi urinary tract disorders secondary to idiopathic hypercalciuria in children. Ped Clin N Am. 1987;34(3):711-8.
- Polito C, La Manna A, Cioce F, et al. Clinical presentation and natural course of idiopathic hypercalciuria in children. Pediatr Nephrol. 2000;15(3-4):211-4.
- Stapleton FB, Roy S 3rd, Noe H, Jerkins G. Hypercalciuria in children with hematuria. N Engl J Med. 1984;310(21):1345-8.
- Kalia A, Travis LB, Brouhard BH. The association of idiopathic hypercalciuria and asymptomatic gross hematuria in children. J Pediatr. 1981;99(5):716-9.
- Roy S, Stapleton FB, Noe HN, et al. Hematuria preceding renal calculus formation in children with hypercalciuria. J Pediatr. 1081;99(5):712-9.
- Vachvanichsanong P, Malagon M, Moore ES. Urinary incontinence due to idiopathic hypercalciuria in children. J Urol. 1994; 152(4):1226-8.
- Parekh DJ, Pope JC IV, Adams MC, et al. The role of hypercalciuria in a subgroup of dysfunctional voiding syndromes of childhood. J Urol. 2000;164(3Pt2):1008-10.
- Escribano Subias J, Vicent Rodriguez M, Feliu Roviva A, et al. Idiopathic hypercalciuria, clinical manifestations, outcome and risk for urolithiasis in children. Ann Esp Pediatr. 1997;46(2):161-6.
- Vachvanichsamong P, Malagon M, Moore ES. Recurrent abdominal and flank pain in children with idiopathic hypercalciuria. Acta Pediatr. 2001;90(6):643-8.
- Vachvanichsamong P, Malagon M, Moore ES. Urinary tract infection in children associated with idiopathic hypercalciuria. Scand J Urol Nephrol. 2001;35(2):112-6.
- Penido MG, Lima EM, Marino VS, et al. Bone alterations in children with idiopathic hypercalciuria at the time of diagnosis. Ped Nephrol. 2003;18(2):133-9.
- Freundlich A, Alonzo E, Bellorin-Font E, et al. Reduced bone mass in children with idiopathic hypercalciuria and their asymptomatic mothers, Nephrol Dial Transplant. 2002;17(8):1396-401.
- Polito C, Iolascon G, Nappi B, et al. Growth and bone mineral density in long–lasting idiopathic hypercalciuria, Pediatr Nephrol. 2003;18(6):545-7.
- Garcia–Nieto V, Ferrandez C, Monge M, et al. Bone mineral density in pediatric patients with idiopathic hypercalciuria. Pediatr Nephrol. 1997;11(5):578-83.
- Tasca A, Cacciola A, Ferrarese P, et al. Bone alterations in patients with idiopathic hypercalciuria and calcium nephrolithiasis. Urology. 2002;59(6):865-9.
- Giannini S, Nobile M, Santori L, et al. Bone density and skeletal metabolism are altered in idiopathic hypercalciuria, Clin Nephrol. 1998; 50(2):94-100.
- Zanchetta JR, Rodriguez G, Negri AL, et al. Bone mineral density in patients with hypercalciuric nephrolithiasis. Nephron. 1996; 73(4):557-60.
- Weisinger JR: Bone loss in hypercalciuria cause or consequence? Am J Kidney Dis. 1999;33(1):46-8.
- Audran M, Legrand E. Hypercalciuria. Joint Bone Spine. 2000;67(6):509-15.
- Aladjem M, Barr J, Lahat E, Bistritzer T. Renal and absorptive hypercalciuria: a metabolic disturbance with varying and interchanging modes of expression, Pediatr. 1996;97(2):216-9.
Copyright 2007 - TUMS PUBLICATIONS
The following images related to this document are available:
Photo images
[pe07066t1.jpg]
[pe07066t2.jpg]
[pe07066t3.jpg]
|

{kind=link}
{kind=link}
{kind=link}