 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 17, No.4, December 2007, pp. 364-368 A 10 Year Survey of Neonatal Kidney Mass in North-East of Iran (Khorasn) Gholam-Ali Mamouri1, MD; Hassan Boskabadi2, MD; Farhad Heydarian*2, MD 1Neonatologist, Department of Pediatrics, Mashad University of Medical Sciences, IR Iran Received: 09/10/06; Revised: 19/07/07; Accepted: 20/10/07 Code Number: pe07068 Abstract Objective: Although abdominal mass in neonates is not common, it is very critical to detect it
promptly. 2/3 of neonatal abdominal masses belong to kidney. Correct diagnosis and immediate
appropriate management can prevent morbidity and mortality. This study pays special attention to
incidence, associated anomalies and mortality rate in those neonates who suffered from palpable
kidney mass. Key Words: abdominal mass, neonate, poly cystic kidney S, multicystic kidneys. IntroductionAbdominal mass is an important problem in neonatal period which should be kept in mind when visiting a newborn baby. It can easily be confirmed by abdominal sonography. After detecting an abdominal mass which mainly has renal origin, it is possible to intervene appropriately to prevent complications. It is estimated that about 1 out of 500 fetuses has nephromegaly.[1] It is possible to detect kidneys in neonates especially prior to pneumatisation of bowels.[2] In a study from France, among 93 prenatal urinary tract abnormalities, the most common one (48%) was hydronephrosis.
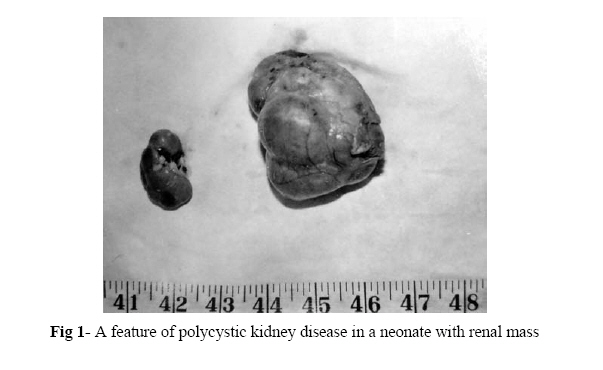
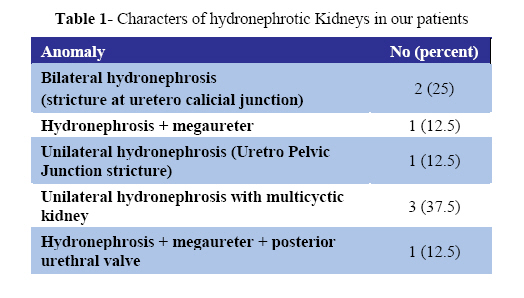
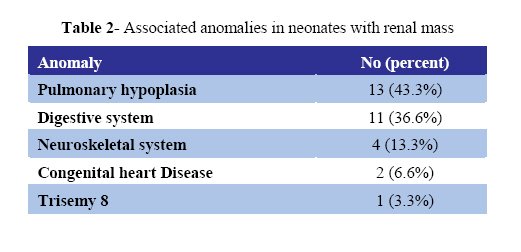
Because of importance of neonatal abdominal masses and lack of studies in north-east of Iran (Khorasan), we arranged this study to show the incidence, types and prognosis of neonatal abdominal masses of renal origin. Material & MethodsIn a retrospective study the records of 48250 live born neonates during 10 years from 1990-1999, in Ghaem hospital, Mashad, were assessed. In 30 cases renal mass was suspected by neonatologists or residents of pediatrics and confirmed by abdominal sonography. In cases of death, autopsy revealed the pathology of the mass. Those who survived were followed up to the age of 28 days. Finally, data was analyzed with statistical measures. FindingsThe incidence of abdominal mass due to renal abnormality was 6.2 in 10000 live births (1/1600 neonates, 30 cases). Among them, 23 (76.7%) cases were born term and 7 remainder (23.3%) preterm. 22 cases (73.4%) were males. Male to female ratio was 2.75/1. The mean (standard deviation) weight of patients was 2946 (436) grs. Apgar score was equal to or above 7 in 20 cases (66.6%), between 3-6 in 8 cases (26.6%) and below 3 in 2 cases (%6.7) 5 minutes after delivery. Abdominal mass was the cardinal sign. Respiratory signs consisting of cyanosis, respiratory distress and apnea also were present in 20 (66.6%) patients. Sonographic and pathologic results demonstrated polycystic kidney disease (PCK) in 16 (53.3%) cases, unilateral multicystic kidney (MCK) in 7 (23.3%) cases (Fig 1), of whom 3 patients had hydro-nephrosis, 5 (16.7%) patients isolated hydro-nephrosis and 2 (6.7%) cases idiopathic nephromegaly. Character of hydronephrosis in 8 cases is shown in Table 1. Associated anomalies in the most of patients were demonstrated by pathologic examination. Table 2 shows these abnormalities. This table shows that pulmonary and intestinal anomalies are the most common abnormalities associated with kidney mass in newborns. Three cases had Potter syndrome and 4 cases suffered from pneumothorax at the first day of life. Totally, 22 (73.3%) cases expired, of whom 13 (59.09%) had PCK, MCK was found in 5 (22.72%) patients and hydronephrosis in 4 (18.18%) cases (autopsy confirmed). The main cause of death in PCK was lung hypoplasia (11cases), followed by multiple anomalies and secondary sepsis. Sepsis and pyelonephritis were the cause of death in 3 cases with hydronephrosis and meningitis superimposed on meningomyelocele in one case. Secondary sepsis and lung hypoplasia in one case and multiple abnormalities were among the etiologies of mortality in MCK patients. Discussion Early diagnosis of abdominal mass is necessary to decrease the morbidity and mortality rate. In our cases the incidence of renal mass was 1 in 1600 live births. It is different from that in other reports (1/500).[1,2] Main cause of this difference seems to be lack of sonography examination prenatally in our study. In other words, we detect the patients after delivery, first with clinical examination of the abdomen. Palpable abdominal mass in neonates is seen in 0.2-0.6% of live births with 70% being of renal origin.[1,4,5] In sonography, MCK can be detected by revealing renal cysts in varying size which have a left side predominancy.[6] In one study from Japan performed on 2700 neonates, 112 (4.1%) cases had kidney anomalies in the first sonography and in 18 (0.67%) cases kidney anomalies were discovered in a second examination. These anomalies consisted of Uretro Pelvic Junction obstruction (UPJO) (7 cases), megaureter (2 cases), and hypoplastic kidney (4 cases).[7] Most of our patients were born at full term, because renal mass in prenatal period plays no significant role in fetal life. Sixty three percent of patients were males; this shows the higher incidence of renal abnormalities in male gender. In order of frequency PCK (53.3%), MCK (23.3%) and hydronephrosis (16.7%) were among the most common causes of abdominal mass in newborns. In a multicentric study, among 191 renal masses in newborns, 74 (39%) cases had hydronephrosis, 59 (31%) cases MCK, 16 (8%) cases PCK and 2 cases idiopathic nephromegaly.[4] In another study on 10000 neonates, 77 had an abdominal mass in whom 57 renal masses were confirmed by IVP. In 16 cases a horseshoe kidney was detected. Other anomalies consisted of intraabdominal kidney (9 cases), kidney agenesis with contralateral renal enlangement (5 cases), PCK (2 cases), MCK (2 cases), one idiopathic renal enlargement and one Wilms tumor.[8] According to other surveys, the most common renal masses in newborns are hydronephrosis and MCK.[1,2,9] In our study PCK was the most common cause of renal enlargement. It may be a result of more familial marriage in our country. Another possibility is that some mildly hydronephrotic kidneys which could be detected by sonography but not with physical examination, were missed. Incidence of MCK is about 1 in 10000 live births.[10] In our study it was 1 in 7000. Forty percent of MCKs are associated with other anomalies. The most important one is UPJO in contralateral kidney. Vesicoureteral reflux is the next common associated anomaly.[11] We found that 43%of our patients had associated anomalies with MCK. We saw isolated hydronephrosis in 5 patients and hydronephrotic contralateral kidney in 3 cases of MCK. The incidence of hydronephrosis in our cases was 1 in 10000, which is lower than in other reports.[1] UPJO and secondary hydronephrosis counted for the most common causes of abdominal masses in newborns.[9] In our patients, there were 2 cases of UPJO and 2 cases of UPJO and PUV (each one a case) with hydronephrosis. In one study 93 newborns that suffered from renal abnormalities, had prenatal diagnosis. (2.8 cases in 1000 live births) of hydronephrosis in 48%, megaureter in 19% and MCK in 16% of cases.[3] In a similar study, in which 10 neonates had prenatal diagnosis of renal anomalies, it was shown that 5 cases had mild hydronephrosis, 2 cases with UPJO, and 3 cases had PUV.[11] According to a 5-year study on 81 neonates who had anomalies of kidney which was diagnosed prenatally, it was demonstrated that 30 cases had hydronephrosis, 21 cases MCK, 15 cases Potter syndrome, 10 patients PCK, 4 cases solitary kidney cyst, and one case prune belly syndrome.[12] In another 15-year survey on 56 newborns with diagnosis of urinary abnormality which was confirmed prenatally, it was revealed that 18 (32%) cases had serious urinary anomalies with lung hypoplasia and oligo-hydramnious who died perinatally. Thirty eight of the newborns had isolated hydronephrosis and MCK, 6 cases had more than one anomaly.[13] In our study, 18 renal anomalies were associated with extra urinary tract anomaly. Lung and intestinal defects were the most common ones. According to autopsy results, lung hypoplasia was the most common cause of death in our patients (14 neonates, 60%). The next common cause of death was secondary infection which was seen in 7 neonates (30%). ConclusionWe found that PCK in our patients was more common than in other studies. It can be as a result of familial marriage occurring more frequently in Iran. It is recommended that in any neonate suspected of abdominal mass, prompt medical work up including sonography of the abdomen be performed. Correctable urinary tract anomalies such as UPJO or PUV should be managed appropriately. Also prevention of secondary infections and respiratory support in case of lung defects should be considered. References
Copyright 2007 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe07068t2.jpg] [pe07068t1.jpg] [pe07068f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}