 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 17, No.4, December 2007, pp. 379-382 Neonatal Ovarian Cyst: A Case Report Fateme Haji Ebrahim Tehrani 1, MD; Zohreh Kavehmanesh* 2, MD; Mahbod Kaveh 3, MD; Fateme Davari Tanha4, MD 1Neonatologist,
Department
of
Pediatrics,
Shahed
University,
Tehran,
IR
Iran 2Pediatric
Gastroenterologist,
Department
of
Pediatrics,
Baqiyatallah
Medical
Sciences
University
Tehran,
IR
Iran 3Pediatrician,
Department
of
Pediatrics,
Tehran
University
of
Medical
Sciences,
Tehran,
IR
Iran 4Gynecologist,
Department
of
Gynecology,
Tehran
University
of
Medical
Sciences,
Tehran,
IR
Iran Received: 12/07/07; Revised: 14/09/07; Accepted: 22/09/07 Code Number: pe07071 Abstract Background: Ovarian
cysts
are
the
most
frequent,
prenatally
diagnosed
intra-abdominal
cysts.
Prenatal
ultrasonography
allows
diagnosis
of
ovarian
cysts
and
may
suggest
antenatal
complications.
The
management
of
fetal
ovarian
cysts
is
still
controversial
despite
the
improvement
in
prenatal
diagnosis
with
ultrasonography.
Some
studies
suggest
an
aggressive
management,
while
others
plead
for
a
conservative
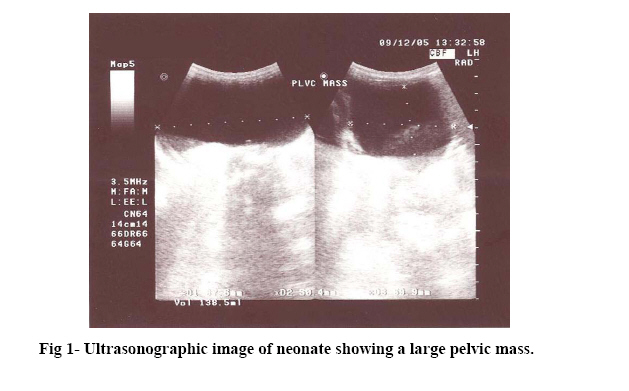
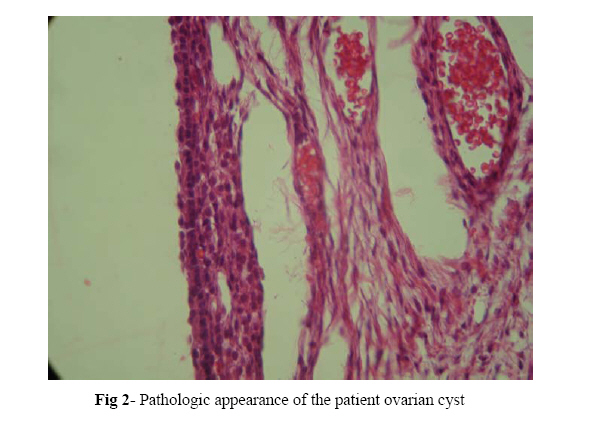
one. Key Words: Ovarian cyst, Abdominal mass, Neonate, Fetal, Abdominal distension IntroductionFetal tumors represent a rare and heterogeneous group of abnormalities[1]. In female newborns, ovarian cysts are the most frequent type of abdominal tumors[2]. The first case of ovarian cyst was reported in 1889 in a stillborn premature. In 1942 Bulfamonte reported the first case of an ovarian cyst successfully treated during the newborn period.[3] The incidence of ovarian cysts has been estimated at more than 30% (this estimate is based on an investigation of stillborns or infants who died within 28 days after birth)[4]. Obstetrical ultrasound provides the opportunity to diagnose ovarian cysts in utero that would otherwise have gone undetected. It also may suggest antenatal complications (visceral compression, polyhydramnios, cyst rupture with hemorrhage and ovarian loss from torsion or autoamputation).[5] An ovarian cyst can be suspected if a fluid-filled structure is visualized next to a fetal kidney and female external genitalia are recognizable. In most cases, the normal course of fetal ovarian cyst is a spontaneous intrauterine or postnatal involution. In the most of cases, the size of ovarian cyst is small, seeming to resolve spontaneously and is of no clinical significance.[6] Fetal ovarian cysts are usually unilateral, diagnosed in the third trimester and are uncommon. Average size of ovarian cysts is 5×5 cm at the diagnosis and this large size doesn’t change throughout the pregnancy. In approximately 30% to 40%, ovarian torsion results, that is an indication for immediate surgical intervention. Large cysts can compress other viscera or rupture can occur. At times hydramnios might occur due to obstruction of the fetal gastrointestinal tract. The etiology of fetal ovarian cysts is still unknown, but hormonal stimulation is generally considered to be responsible for the disease[2]. Most cysts are functional in origin and histologically benign simple cysts.[7] The association of fetal ovarian cysts with maternal diabetes or fetal hypothyroidism has been described.[8,9] We searched for any report of ovarian cyst in neonates from Iran in Pubmed, Iranmedex and Iranian Scientific Information Database and didn’t find any report of neonatal ovarian cyst in the literature from Iran. Thus, this case is the first ovarian cyst successfully treated in a newborn from Iran. Case PresentationA 29 year-old mother, gravida 2, with a history of an abortion and hypothyroidism treated with Levothyroxin for 3 years lasting till one year earlier, delivered with cesarean section (repeat cesarean) in Khatam-ol-Anbia hospital in Tehran. Fetal ultrasonography had shown an abdominal thin walled 6×7 cm cyst superior to the bladder (probable ovarian cyst). Her female newborn weighing 2800 grams had gestational age of 38 weeks and Apgar scores of 9 and 10 (after 5 and 10 minutes respectively) with respiratory distress due to severe abdominal distension. Her chest radiography was normal. She didn’t have any other anomaly except for III/VI systolic murmur in left sternal border; echocardiography showed a small VSD, ASD and PDA. Serum electrolytes, blood sugar and calcium were normal. Thyroid function tests were normal. Postnatal abdominal ultrasonographic scan revealed a cystic mass 88×50×60 mm in left ovary (Fig 1) Due to large size of ovarian cyst laparotomy and cystectomy of the left ovary was done. Pathologic examination revealed a large white yellowish cystic mass 90×60×60 mm with thin border filled with serous fluid as simple ovarian cyst (Fig 2). On the third day after surgery she had an uncomplicated post operative course and was discharged in a good general condition. DiscussionOvarian cysts are the most frequent, prenatally diagnosed intra-abdominal cysts.[2] The most appropriate clinical approach in the management of benign feto-neonatal ovarian cysts is to adopt a wait-and-see policy, assessing the course of the condition by means of periodic ultrasound monitoring. Spontaneous resolution of cysts <3 cm is not uncommon both prenatally and after delivery. Some suggest, however, aspiration of the cystic contents is possible even in ovarian cysts exceeding 4 cm in diameter.[7] Prenatal diagnosis improves neonatal outcome by allowing an appropriate choice of the optimal time, mode and place of delivery in order to avoid accidental and unexpected intrapartum and postnatal complications. The management of a fetus affected by an ovarian cyst depends on the size and on the echopattern of the cyst. Some recommend intrauterine aspiration of the cyst to be attempted in the presence of large cyst filling the fetal abdomen. Bagolan et al have reported their experience on fetal ovarian large simple cysts with aspiration in utero. They performed prenatal aspiration in cysts over than 5 cm diameter. They suggest that prenatal aspiration of ovarian cysts appears effective and safe. They also recommend surgical management for cysts with ultrasound pattern of torsion persisting postnatal.[10] Heling et al reported 64 fetal ovarian cysts. These ovarian cysts were identified during prenatal sonography at 26 to 40 weeks gestation (median 35 weeks). They reported spontaneous resolution in 34 cases (parentally in 18 and postnatally in 16).[7] Approximately half of the neonates underwent surgical resection for various indications (increase in size, clinical suspicion of torsion, intracystic hemorrhage, clinical symptoms of an ileus, and suspicion of teratoma). At surgery, one mass turned out to be a teratoma.[10] Kwak et al reviewed 17 cases of fetal ovarian cysts diagnosed since 1990 to 2005 from Korea. Postnatal surgery was performed in 7 infants. Four cases of ovarian cyst torsion were confirmed. In the remaining 10 fetuses, one case regressed completely during pregnancy, and the other nine cases including two complex cysts resolved spontaneously after birth. Postnatal symptomatic cysts or cysts with a diameter greater than 5 cm that do not regress or enlarge should be treated, but uncomplicated asymptomatic cysts less than 5 cm in diameter should only be observed and reassessed by serial ultrasonography. If they regress spontaneously, no surgical intervention is necessary independent of their sonographic findings.[6] Kwak et al reported two cases of large ovarian cysts treated by ultrasound guided puncture before delivery and both fetuses underwent surgery later without complications. If properly performed, puncture of the cyst seems to be a low risk procedure in comparison to potential problems that cyst may cause to the fetus or by causing dystocia. Ultrasonographic-guided aspiration of large neonatal cysts preserves ovarian tissue in a higher percentage of patients than surgery. It is safe, effective, and repeatable. Kessler et al recommend US-guided aspiration of asymptomatic large ovarian cysts for salvage or for decompression if intrauterine ovarian torsion occurs. They believe surgery should be reserved for patients with acute torsion, intestinal obstruction and intestinal volvulus.[11] Simple ovarian cysts may be treated with fenestration of the cyst or cystectomy. Complex cysts should be treated with cystectomy when possible to avoid unnecessary loss of functional ovarian tissue. In cases where no viable tissue remains, oophorectomy may be necessary.[5] Even though the relation of neonatal hypothyroidism and ovarian cyst has been reported earlier[9], we didn’t find any relation between maternal hypothyroidism and neonatal ovarian cyst. Our patient had additional cardiac findings, but we didn’t find any relation between congenital heart diseases and ovarian cyst in literature. ConclusionNeonatal simple ovarian cysts are rare, but may cause abdominal distension, and other complications. A wait and see policy is recommended in cases of small size ovarian simple cysts, surgical intervention is reserved for complicated or large size ovarian cysts. References
Copyright 2007 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe07071f2.jpg] [pe07071f1.jpg] |
| |||||||||

{kind=link}
{kind=link}