 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 18, No. 1, March, 2008, pp. 57-61 Short Communication Comparison of Sacral Ratio in Normal Children and Children with Urinary and/or Faecal Complaints Abdol Mohammad Kajbaf Zadeh*1, MD, Pediatric Urology; Farideh Nejat2, MD, Neurosurgeon; Parvin Abbaslou, MD, Fellowship in Pediatric Gasteroentrology 1
Department of
Urology, Tehran University of Medical Sciences, IR Iran Received: 23/09/07; Revised: 27/12/07; Accepted: 08/02/08 Code Number: pe08009 Abstract Objective: Sacral ratio (SR) measurements in
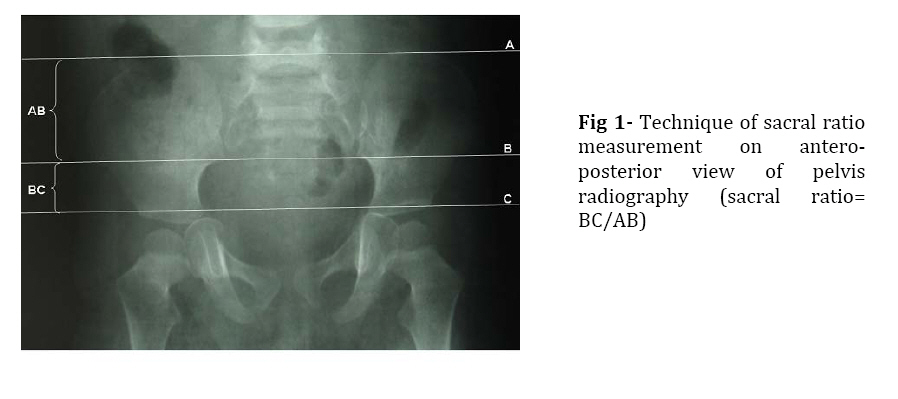
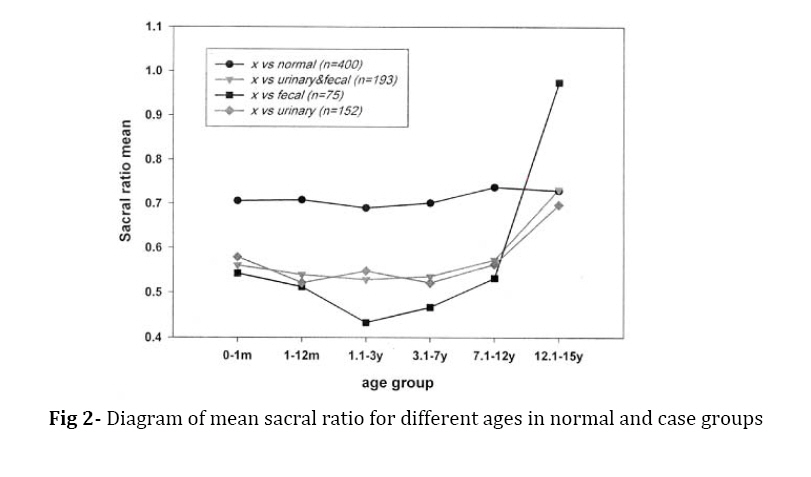
children with urinary and faecal complaints is less than that in normal children. Key Words: Children, Faecal complaints, Sacral ratio, Urinary complaints IntroductionSacral anomalies and low-length sacrum have been explained previously in anorectal malformation (ARM)[1-4]. In 1995 Pena[2] proposed a bony index called sacral ratio (SR) as a form of evaluation of sacrum in patients with ARM. He suggested that it could be a useful method by which we can estimate the final functional prognosis in these patients, based on the fact that bone abnormalities could be accompanied by changes in lumbosacral spine innervation. Patients with urinary and/or faecal complaints but without any structural or known neurogenic disease compose a group, in which the prognostic factors are not well recognized. Radiography of pelvis is a common imaging modality in evaluating these patients and in our pediatric urology clinic. We have observed decreased length of sacrum or sacral agenesis as a frequent finding. Sacral dimensions might be used as probable prognostic value in the patients. Accordingly, we evaluated SR as a measure of sacral development in these patients and compared it with the measurements in a large group of normal children which was not reported previously. Material & Methods We performed the current study at Children’s Medical Center in Tehran University of Medical Sciences from April 2002 through 2003. Five hundred ninety four children aged less than 15 years with abdominal plan or pelvic x-ray for different reasons at this period, were included. SR was measured in anteroposterior radiography (APSR) with patient lying supine and the knees were not bent. 193 patients with urinary and/or faecal complaints who had no structural abnormalities in the urinary or nervous system were studied. One hundred seventeen (60.6%) patients had only urinary complaints including dysuria, frequency, nocturia, recurrent UTI, diurnal incontinence, urgency, and/or dribbling, 40 (20.7%) had only faecal problems including faecal incontinence and/or constipation, 36 (18.6%) had both complaints. APSR was also measured in 401 children undergoing pelvic radiography for diverse reasons such as trauma, hip problems, arthritis, back pain, urinary lithiasis, appendicitis and abdominal pain who had no history of urinary or faecal complaints. All children with any known neurogenic disease, myelodysplasia, cloacal exstrophy, Hirshsprung`s disease, ARM, and scoliosis were excluded from the study. Moreover, all children with inappropriate radiography were not included. To calculate the SR from plain lumbosacral spinal images in the antroposterior view, a line is drawn joining the most superior points of both iliac crests. The second line is located from the lowest point of one of the posterior and inferior iliac spines to the other. A third line runs parallel to the other two lines and touches the lowest radiologically visible point of the sacrum (Fig.1). The SR is then obtained by dividing the distance between the two lower lines by the distance between the two upper lines.[1] All images were studied by the same observer. In order to correlate SR values with all data, linear regression test and Pearson`s r-correlation test were used. Analysis of data was performed by SPSS software. With the hypothesis that SR values are lower in case were one tailed. Moreover, all tests group than in normal group, all statistical tests were carried out with an a=0.05 level of significance. Findings Children were 52.2 % male and 47.5% female. The most common complaints in urinary group were recurrent urinary tract infections and nocturnal enuresis. In faecal group the most common complaints were constipation and faecal incontinence. The average APSR in normal group was 0.71 with a range of 0.36 to 1.333. The mean APSR in urinary group was 0.55 with a range of 0–1.0 and in faecal group 0.491 (range 0-0.97). In urinary and/or faecal (case) groups the mean APSR was 0.554, ranging between 0 and 1.0. There was no statistically significant difference between males and females with APSR in either group (t-test P=0.7). SR was categorized into 3 limits, less than 0.4, between 0.4 to 0.7 and more than 0.7. This subdivision was evaluated in all groups. Moreover, the comparison in each category between the cases and normal group was performed. As a result, There were significant differences between the case and normal groups according to subdivided SR values (P<0.001). Mean SR was evaluated in normal and case groups for different age categories including neonates (up to 1 month), infant (1-12 months), toddler (1.1-3 years), preschool age (3.1-7 years), school age (7.1-12 years) and adolescence (12.1-15 years). The curve of average SR and age in normal group (Fig.1) showed no obvious steepness, there was almost a plateau and insignificant difference between mean SR in different age groups (P>0.05). Interestingly enough, the average SR curve in case group had an obvious slope with increasing age to adolescence period (Fig. 2), with a statistically significant difference between age categories (P<0.001). Sacral agenesis as the absence of a part or all of the two or more sacral vertebral bodies has been studied in this research. None of children in the normal group and 13.3% in the case group had sacral agenesis. The difference between the two groups regarding sacral agenesis was statistically significant (P<0.001). Discussion Pena introduced SR in ARM, based on the fact that bone abnormalities would almost always be accompanied by changes in lumbosacral spine innervation[2]. Patients who had short sacrum on radiological view would be those most likely to have a neurological disorder capable of irremediably comprising the sphincter activity[2]. There are other studies that discussed SR values in ARM[1-4]. Torre et al and Oh JT et al evaluated SR in normal children.[3,5] There are limited reports in children with vesicoureteral reflux and persistent primary enuresis that have shown SR as a cardinal index in the prognosis of children with urinary and/or faecal abnormalities[7,8]. We are often confronted with sacral abnormalities during the assessment of patients with urinary and/or faecal complaints. These observations prompted us to find some parameters related to sacrum that could confirm that this association is not incidental and somewhat explains the underlying pathophysiology. Due to some similarities between ARM and our patients in sphincter related symptoms we used SR values and tried to correlate SR values with age, sex and compare them between case and normal groups. In the normal population mean APSR was 0.711, similar to those reported in the literature.[2-5] However we found that SR can have a wide range of values in normal population (0.36–1.333). All children in normal group had an APSR value more than 0.40 except for one with the value of 0.36. Pena considered APSR value of less than 0.40, a pathological value[2] andTorre et al considered it below 0.52 frankly pathologic[3]. It is emphasized that there is no case with SR value less than 0.3, who had a good bowel function[1]. We showed that there are no normal children with good urinary and faecal function but with SR value less than 0.36. The lower limit of APSR value in our case group is zero. In the normal group 0.3% of children had SR less than 0.40, but in the case group 17.2% of patients had SR less than 0.40. So we agree with Pena and consider the SR value less than 0.40 as a pathologic value. Age seems to be a probable parameter influencing SR. Oh JT et al observed no correlation between SR and age in their patients[3]. We found SR tended to increase with age in case group while it did not change significantly in the normal group (Fig. 2). Our study with a great number of normal children could not show any difference in mean APSR in the normal group but Torre et al had shown an increase in SR value with growth in normal children and a decrease in SR value with age in children with ARM. The possible reason for this observation was that the sacrum in their patients is congenitally involved and can not grow proportionally with the child pelvic bones. Congenital sacral involvement thus becomes more evident at an older age and is evidenced by a decrease in SR[3]. Our patients with urinary and/or faecal complaints had shown a slope in the curve of SR average in adolescence. This slope can be explained only in the case group and not in the normal group by the growth and maturation of bony skeleton with age. Some authors showed improvement of vesicoureteral reflux and competence of ureterovesical junction over time can count as a measure of skeletal maturity[9]. Children with urinary and/ or faecal complaints have the compliance of sacral growth appropriately and we can observe its probable evidence in gradual improvement of some of their complaints in adolescence or puberty. The lateral SR is measured similar to anterior–posterior sacral ratio (APSR) but since the pelvis AP view is perfomed much more frequently than the lateral view especially in the normal group we had to use the AP view for our study. We have not found any data in the literature that could explain SR values in patients with urinary and/or faecal complaints but without any structural or known neurogenic disease. So far, ranges of variablity of SR in normal children and average normal values at different ages have not been reported in a great population number. Oh JT et al evaluated the SR in normal children and in children with ARM and confirmed a significantly lower SR in these patients[3]. Torre et al reported SR values in 147 normal children aged 0-14 years and determined its normal range[5]. Conclusion The antero-posterior SR has a wide range of normal values (0.36-1.33). The average APSR in the normal child was 0.71 and in children with faecal and/or urinary complaints was 0.55. The APSR should be considered abnormal when it is less than 0.4. Sacral hypoplasia can be associated with involvement of spinal cord and pelvic innervations and can be associated with poor functional status. The average APSR increased over time in the case group which is an indication of gradual maturation and could explain the cessation of vesicoureteral reflux in some cases. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08009f1.jpg] [pe08009f2.jpg] |
| |||||||||

{kind=link}
{kind=link}