 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 18, No. 1, March, 2008, pp. 67-70 Case Report Hydrometrocolpos Due to Persistent Urogenital Sinus Mimicking Neonatal Ascites Rizwan Ahmad Khan*1, Senior Resident, Pediatric Surgery; Imran Ghani1, MCh, Professor, Pediatric Surgery; Shagufta Wahab2, Senior Resident, Radiology 1Division of Pediatric
Surgery, Department. of Surgery, JNMCH, Aligarh, India Received: 12/07/07; Revised: 17/12/07; Accepted: 26/12/07 Code Number: pe08011 Abstract Objective: A urogenital sinus is
a common channel into which both the urethra and genital tracts open.
Occasionally there might be transverse obstructing membrane leading to
hydrometrocolpos from either uterine secretions or urine. Although the
presentation is varied, a neonatal presentation of a large hydrometrocolpos
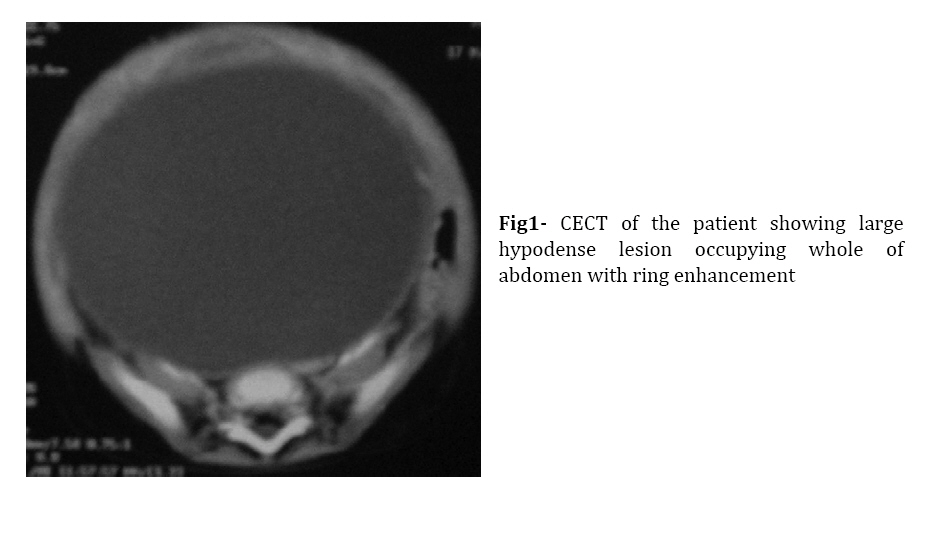
mimicking gross ascites is rare. Key Words: Hydrometrocolpos, Urogenital sinus, Neonatal ascites Introduction Hydrometrocolpos is cystic dilatation of the vagina and uterus due to congenital vaginal obstruction. It may be secretory or urinary in character and manifests in the neonatal period with abdominal distension. Congenital obstructing lesions of vagina leading to hydrometrocolpos, and hematocolpos, present at a variable time during early childhood and adolescence to different medical and surgical specialties. Urogenital sinus is an important, but often missed, cause for hydrometrocolpos[1]. Large hydrometrocolpos can present as tense ascites and therefore attending clinician must be inclining to such a possibility thereby preventingthe morbidity associated with delays in diagnosis, includingthe rapid progression of symptoms as in our case. We present an unusual presentation of a patient of hydrometrocolpos. Case Presentation A 3-day-old female neonate was born at term gestation by vaginal delivery with no history of birth difficulty. 1-min Apgar score was 8. Antenatal history did not reveal exposure to teratogen, infection or diabetes. There was no family history of similar disorder. At birth patient had gross abdominal distension but there were no features suggestive of bowel obstruction. Urethral catheterization was not successful. Abdominal X-ray and ultrasonography done outside revealed findings of ground glass appearance and gross ascites respectively. At presentation the baby was well hydrated and her cry, tone and activity were fairly good. Per abdomen examination revealed generalized distension with some prominent veins. Fluid thrill was present and bowel sounds were heard well above in both hypogastric regions. Perineal examination revealed a single opening in the introitus region and a normally placed anal opening. Patient was investigated and her laboratory investigation revealed white cell count to be 14.5x103/mm3 and hemoglobin was 17 g%. Patient was subjected to CECT abdomen. It revealed a large hypodense lesion posterior to urinary bladder and anterior to rectum occupying whole of abdomen with a possible origin from pelvis (Fig 1). Based on clinical and CT findings patient was taken up for exploratory laparotomy. Her operative findings were a hugely distended vagina with uterus lying over it. Rest of the abdominal viscera was normal. Tube vaginostomy was done. It drained about 200 ml of brownish fluid. In the postoperative period patient progressed well and vaginostomy drain was removed on 25th postoperative day. Thereafter the patient was in follow-up and patient remained stable. Patient has been planned for definitive repair in future. Discussion The common urogenital sinus is a normal stage of embryonic development in both sexes. The persistent urogenital sinus with common channel for the urinary and genital tracts in female represents developmental arrest after the paramesonephric duct has fused with the urogenital sinus at about 9 weeks of gestation before the urogenital septum has migrated to divide the urinary and genital tracts[2]. A long urogenital sinus with a short vagina and a high urethral opening results when the defect occurs at an early stage. A short urogenital sinus with almost normal length vaginal vestibule and low urethral opening results when the defect occurs late in the development[2]. Common presentations in neonates can be asymptomatic, abdominal mass, neonatal sepsis, and respiratory distress. It may also present as hydronephrosis[3] or peritoneal calcification[4]. The abdominal lump is due to the distended vagina (hydrocolpos) or vagina and uterus (hydrometrocolpos). Vaginal and cervical epithelium secretes mucus in response to maternal estrogens. This pools in the obstructed vagina. The distended vagina may press on the bladder outflow causing obstructive uropathy with hydroureteronephrosis or urinary infection. There are other causes of hydrometrocolpos which need to be ruled out. Imperforate hymen is uncommon, occurring in 0.1 % of newborn females[5]. It presents usually in the adolescent period with primary amenorrhea, cyclic abdominal pain or hematocolpos. Less often it may present in neonates or infants with an abdominal lump and an interlabial bulging membrane[6] or causing severe renal compromise and abdominal ascites.[7]The true incidence of these anomalies is unknown but is reported between 0.1 and 3.8%[2].Neonatal urinary ascites caused by bladder perforation is rare[8,9]. The diagnostic approach is based on good clinical evaluation especially thorough perineal examination and adequately defining the anatomy with the help of CT scan and retrograde dye study[10]. Endoscopy is particularly helpful in defining the length of urethra especially in patients with long common channel. The high vagina usually drains well via a urogenital sinus and rarely pools sufficient urine to be a source of infection or interfere with normal bladder emptying[11]. Hydrocolpos and hydrometrocolpos may be associated with other malformations, such as postaxial polydactyly, anal atresia, esophageal atresia, renal agenesis, genital anomalies, and cardiopathy. Each neonate presenting with hydrocolpos should be evaluated for other clinically silent malformations, such as hamartoblastoma of the hypothalamic region[12]. Rarely, symptoms of hydrometrocolpos may manifest antenatally. It should be considered systematically when an ascites, multicystic pelvic mass, bilateral hydronephrosis, abdominopelvic cystic mass is diagnosed in a female fetus. Because the prognosis and neonatal management of isolated hydrocolpos with spontaneous resolution differs greatly from that of hydrocolpos associated with a cloacal malformation, it is important to ascertain prenatally whether there are associated anomalies. Antenatally presence of a fluid-debris level inside the cystic anechoic mass must be considered a crucial finding. Multiple echoes are due to vaginal secretions. This finding must alert the treating clinician to presence of the anomaly before hand[13]. If a patient presents with such a gross abdominal distension due to urogenital sinus then initially laparotomy is indicated with the aim to achieve the vaginal drainage and relieve the symptoms. Recently laparoscopy has come up as the option for diagnostic and therapeutic purposes but the optimal timing of the procedure still needs to be established.[14] Subsequently patient can be taken up for total urogenital mobilization via a posterior sagittal approach for repairing short and long common channels. If the urogenital sinus is low, with a short common channel, a simple U-flap vaginoplasty will be effective[10]. If the vagina enters the urogenital sinus too high up, a division of vaginal moiety from the sinus will be required together with pull through vaginoplasty. Some patients with a long common channel may require additional maneuvers after mobilization to complete the reconstruction for example construction creation of neourethra from anterior vaginal wall.[10]A good surgical correction should provide an adequate vaginal opening into the perineum, create a normal-looking vaginal introitus, fully separate the urethral from the vaginal orifice, remove phallic erectile tissue while preserving glandular enervation and blood supply, and preventing urinary tract complications[15]. Conclusion The diagnosis of hydrometrocolpos should no longer be difficult to determine. Although the rarity and variable presentation can lead to delayed diagnosis and erroneous management, the attending clinician should consider it as differential diagnosis if a female neonate is brought with large abdominal mass. The most important step is a thorough perineal examination, although modern cross-sectional imaging and dye studies help in early diagnosis and delineating the exact anatomy as well as detecting associated renal anomalies. A comprehensive management is necessary to give good cosmetic appearance and to preserve the reproductive potentials. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08011f1.jpg] |
| |||||||||

{kind=link}