 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 18, No. 1, March, 2008, pp. 83-86 Case Report Primary Cerebral Hydatid Cyst: Two Cases Report Farid Radmenesh1, Research Assistant; Farideh Nejat*2, MD, Neurosurgeon 1Tehran University of Medical Sciences, Tehran, IR Iran Received: 18/01/07; Revised: 06/05/07; Accepted: 12/07/07 Code Number: pe08015 Abstract Objective:Cerebral
hydatid disease (CHD) is a rare manifestation of echinococcosis but it
constitutes a significant fraction of all intracranial mass lesions. In this
paper we have reported two children with primary CHD without associated
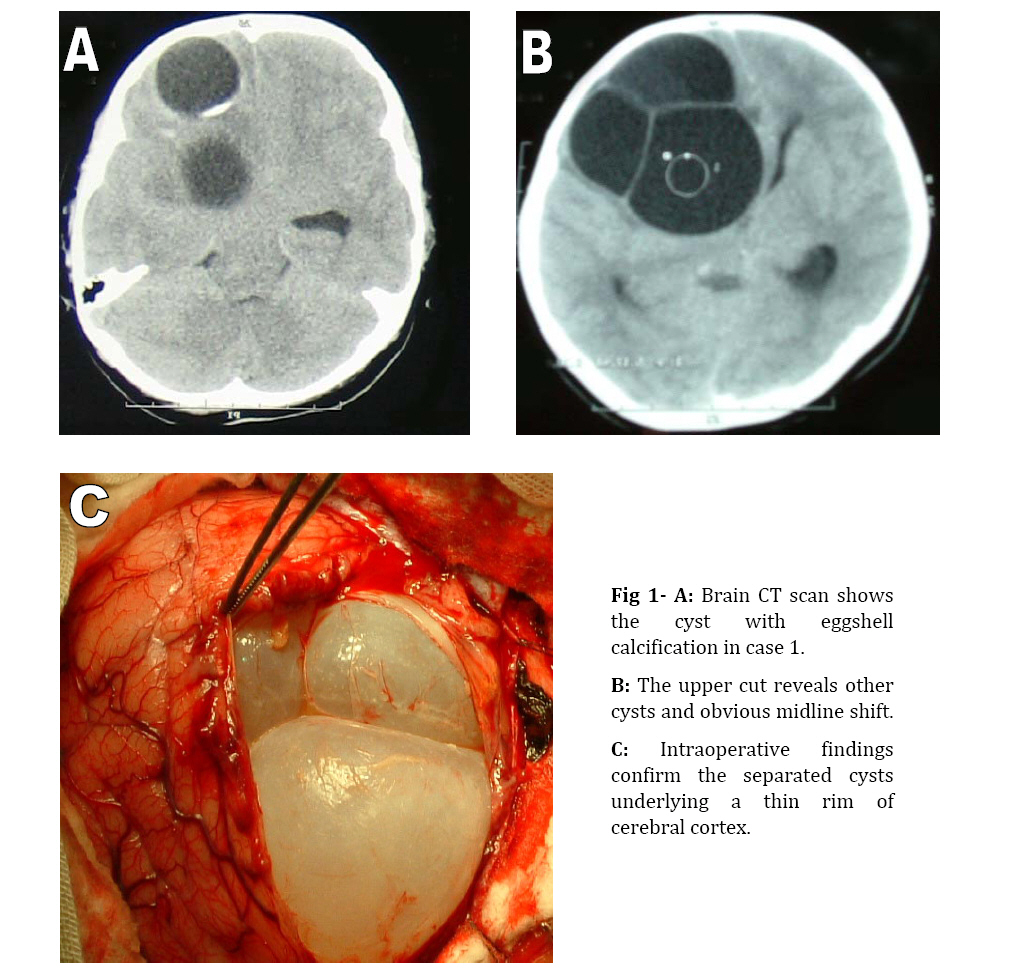
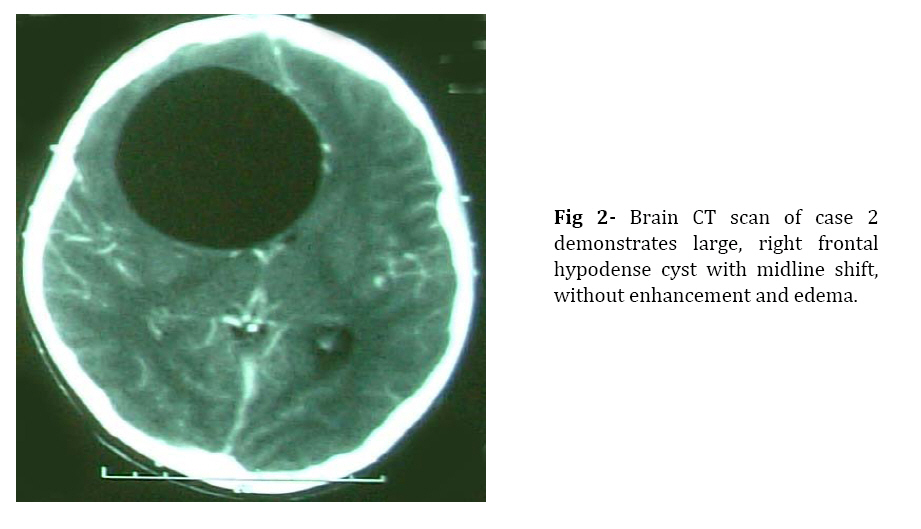
extracranial lesions. Key Words:Isolatedcerebral hydatid cyst; Children; Extracranial Introduction Cerebral hydatid disease (CHD) is a rare manifestation of echinococcosis but it constitutes a significant fraction (1-10%) of all intracranial mass lesions. Fewer than 20% of patients with intracranial hydatidosis demonstrate other organ involvement[1]. The exact pathogenesis of isolated cerebral hydatid cysts is unknown. Here we report two children with primary CHD without associated extracranial lesions and explain some possible mechanisms for this kind of presentation. Cases Presentation Case1: A 7-year-old girl from Afghanistan was admitted because of headache, vomiting and progressive hemiparesis. She had been well until one month earlier. On physical examination, she was conscious but aphasic with bilateral papilloedema and severe right-sided hemiparesis. Routine laboratory tests were all normal. Brain computed tomography (CT scan) revealed large, non-enhancing, well-circumscribed hypodense lesion within left frontal lobe containing four cysts separated by thin septums (Fig 1a, and b). There was no edema surrounding the lesions. Eggshell calcification surrounded the mass in its deepest part. The lesions were diagnosed as hydatid cysts. Casoni’s test and complementary fixation test were negative. She was living in rural areas and had a history of contact with stray dogs. The lesion was removed by a large left frontal craniotomy without intraoperative rupture. Pathological examination confirmed hydatid cysts. CT scans of the thorax and abdomen failed to show any lung or liver lesions. Albendazole was administered for one month. The postoperative period was uneventful until one month later when she developed signs and symptoms of increased intracranial pressure. Brain CT scan revealed obstructive hydrocephalus (triventricular) without recurrence of primary disease. Her symptoms were resolved by ventriculoperitoneal shunting. Two years after surgery, she remained well and free of disease. Case 2: A 12-year old boy was admitted because of five-week history of headache and vomiting. Physical examinations were normal except for bilateral papilledema. Brain CT revealed a large, well-defined cystic lesion in the right frontotemporal region without any surrounding edema and enhancement. Radiological investigations of thorax and abdomen disclosed no evidence of hydatid disease. Serologic tests for hydatid disease were negative. There was a positive history of contact with dogs. The lesion was removed en-bloc through a large frontal craniotomy. Albendazole was administered for one month. He remained disease-free at the end of one-year follow-up. Discussion Hydatid disease or echinococcosis is caused by infection with the larval stage of tapeworm echinococcus. The main pathogenic species for humans are E. granulosus and E. multilocularis, which produce cystic lesions and invasive solid lesions, respectively[2-5]. All organs could be affected, with brain being involved in only 1-2% of all infections[4,6-9]. CHD are 2-3 times more common in children than in adults[1,7,9]. Ninety percent of cases have solitary lesion[10]; most frequently supratentorial, intraparenchymal and in the middle cerebral artery territory[4,11-13]. The diagnostic tools including CT and MRI lead to early and correct preoperative diagnosis. The usual appearance is a large intraparanchymal, non-enhancing hypodense lesion with a well-circumscribed border and no pericystic edema[3,11.12,14]. There are some debates regarding the association of CHD with extracrnial cysts, a number of studies agree with high percentage of other organ involvement[4,6], whereas others do not[1,10]. Ameli and Abbassioun stated that 80-90% of CHDs were accompanied by involvement of other organs in postmortem examinations while in clinical practice, concomitant extracranial cysts were not often demonstrated[10]. The cases reported here, with isolated CHDs support the latter. It has been postulated that infection occurs early in childhood[10,15]. Since brain has a softer tissue, a hydatid cyst in brain grows faster than in other organs. Thus, when hydatid cyst of the brain is large enough to produce symptoms, the cysts in other organs are too small to be detected by clinical and radiological evaluations. Some of these small cysts may not be discovered until 20 to 30 years after the diagnosis of CHDs[10]. Furthermore, diagnosis of CHD usually requires postoperative medication that can eradicate the possible small cysts in other organs. Moreover, immune system can inhibit the growth of larva in other sites except for CNS due to limited access to immune system. In addition, the presence of patent ductus arteriosus, which might remain for several months after birth, can explain why primary cerebral hydatid disease is more common in childhood[6,8,15]. A similar role could be assumed for patent foramen ovale, which is present in 25-30% of individuals[16] and suggested as the potential source of cryptogenic emboli to brain. Conclusion Isolated CHD can occur with different mechanisms. Lack of effective immune system in the brain, the special architecture of brain tissue permitting rapid growth of cyst, patent ductus arteriosus, and patent foramen ovale, have been the proposed factors, but none of them has been proved yet. Further studies are needed to elucidate the exact pathogenesis. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08015f2.jpg] [pe08015f1.jpg] |
| |||||||||

{kind=link}
{kind=link}