 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 18, No. 1, March, 2008, pp. 87-91 Case Report Intestinal Malakoplakia in Children Fatemeh Farahmand*1, MD, Pediatric Gastroenterologist; Hassan Karamy 2, MD, Pediatric Gastroenterologist; Fatemeh Mahjoub3, MD, Pathologist 1Department of Pediatrics, Tehran University of Medical Sciences, IR Iran Received: 16/06/07; Revised: 14/10/07; Accepted: 17/11/07 Code Number: pe08016 Abstract Objective: Malakoplakia is a rare inflammatory disease, related to
enterobacterial infection in the context of a disorder of cell-mediated
immunity. Malakoplakia is exceptional in children and usually involves the
gastrointestinal tract. The diagnosis is exclusively based on histological
analysis. Key Words:Bloody diarrhea; Children; Intestine; Malakoplakia; Pathology Introduction Malakoplakia, (from Greek, “malakos”, soft and “plakos” plaque) is a rare inflammatory disease, related to enterobacterial infection in the context of disorders of cell-mediated immunity. It was initially described in 1902. It has the clinical aspect of a yellow–brown, soft plaque of variable size characterized by a central navel or ulcer and an intense peripheral hyperaemia, usually located in the urogenital and gastrointestinal tract (GIT). These lesions may be solitary, multifocal, or present as a large mass. The clinical presentation of malakoplakia depends on the location of the disease[1-3]. GIT malakoplakia involves mainly the rectosigmoid and proximal colon. There is a slight male predominance and occurs in the age range from 6 weeks to 88 years. Of importance is frequent coexistence of GI malakoplakia with colon cancer[4,5]. Malnutrition, immune suppression, and chronic infection, are other underlying conditions. Clinical picture of colonic malakoplakia depends on the extent of involvement. Commonly reported symptoms include fever, abdominal pain, chronic bloody and mucus diarrhea or hematochezia. Physical signs may include palpable rectal mass, digital clubbing and weight loss. At colonoscopy, the mucosa may have only a nodular appearance or show a hyperemic area covered with necrotic material. Correct diagnosis usually results from examination of biopsy material that contains Michaelis-Gutmann inclusion bodies which typically stain positively with periodic acid Schiff stain[1,2,6]. For treatment diffuse GI involvement, intracellularly active broad-spectrum antibiotics (ciprofloxacin, TMP-SMX, rifampin) are warranted. Cholinergic drugs such as betanchol chloride and also possibly ascorbic acid may be considered but with limited expectation for a favorable result[2,4,5]. Cases Presentation Case 1: A 7-year old girl was admitted with a history of diarrhea for 3 years. Diarrhea was bloody and mucoid, and occurred 4-5 times daily. In physical examination the patient was cachectic and her height was 106 cm (<3rd Percentile, -2SD). Other findings consisted of: abdominal distention, disseminated maculopapular rash on the skin of the abdomen and extremities and digital clubbing. No organomegaly was detected. Developmental state was normal. Perianal area was normal. Case 2: The 9-year old boy was admitted with a history of abdominal pain, intermittent diarrhea, vomiting, anorexia, rectal bleeding, and weight loss for 3 months. On physical examination the patient was lethargic and pale with mild abdominal distention and tenderness. His weight was 15.5 k (<5%) and his height 125 cm <25%. No organomegaly was detected. Perianal area was normal. His sister had also Malakoplakia and died at the age of 15 years old. Case 3: A 7-year old girl with rectal bleeding, anemia, abdominal pain and failure to thrive (FTT) since 5-6 months ago was referred to Table 1- Laboratory test results in 3 patients with malakoplakia
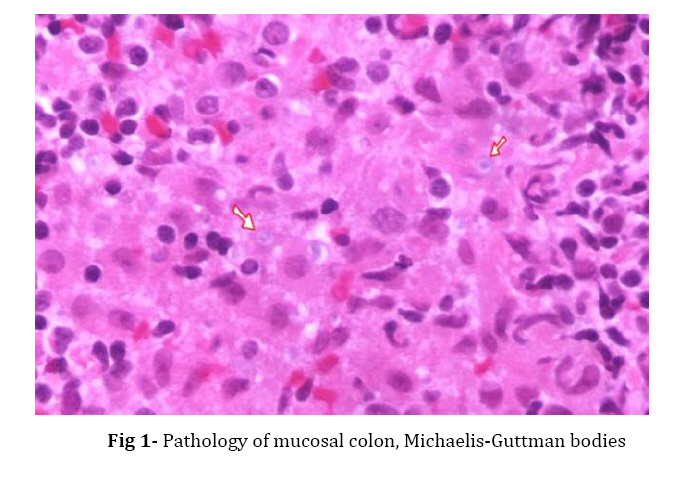
Children’s Medical Center. On admission she had high blood pressure, (140/90 mmHg, more than 95th percentile for age), was lethargic, with mild abdominal distention and pallor. She weighed 15 kg (<5th percentile, - 2SD) and her height was 122 cm (<25th percentile). A digital clubbing was not present. Laboratory test results of all 3 patients are present in table 1. Abdominal sonography in all 3 patients was normal. In case 1 small bowel barium flow-through, demonstrated a nodular pattern from ileum through cecum with cecal deformity. Upper endoscopy was normal in all 3 patients, but gastric biopsy in one case, detected severe chronic gastritis with helicobacter pylori (HP). Histology of small intestinal biopsy was normal in all patients. In one case colonoscopy showed yellow nodular lesions in the left colon, with erythema and edema of the mucosa, pseudopolyps and superficial ulcers. Colon biopsy showed colonic mucosa with infiltration of large macrophages in lamina propria with abundant pink cytoplasm, containing typical Michaelis-Guttman bodies and also infiltration of lymphomononuclear cells (Fig. 1). Treatment consisted of trimethoprim-sulfamethoxazole, vitamins and trace elements for 3-4 weeks. All 3 patients responded favorably. Although the response to therapy is unpredictable, these patients responded to it. They were well in follow-up visits; the treatment was planned to be continued for a long term. Discussion Malakoplakia is an uncommon granulomatous inflammatory disease most commonly found in the bladder and the rest of the urinary tract. It has been also seen in other locations, including colon, liver, joints, skin and brain.[8] There are approximately 500 cases reported worldwide since 1902[1,3]. Malakoplakia is usually associated with Klebsiella and Escherichia coli, although gram-negative and gram-positive cocci and acid fast bacilli have also been identified. Recently, malakoplakia is reported to occur in association with unusual organisms such as Rhodococcus equi and Paracoccidioidomycosis infection[7]. The most plausible pathogenic explanation for the development of malakoplakia centers on the defective function of macrophges that phagocyte the bacteria but are unable to kill or digest them. Intracytoplasmic phagolysosomes continue to enlarge and coalesce with subsequent degenerative change of both matrix and limiting membrane. The deposition of crystals within enlarged phagolysosome leads to the development of the characteristic, concentrically laminated Michaelis-Gutmann inclusion bodies[8,9]. In this study, all 3 cases had colon malakoplakia. In one of the cases it was located in the rectum, sigmoid and descending colon, while in the other two cases the lesion was located in the rectum. Malakoplakia had been diagnosed in the older brother of the second case in this study. Mouzan et al reported two brothers in a family with documented colonic malakoplakia[10]. Marino and coworkers reported 5 children with intestinal malakoplakia from Mexico during a period of 10 years (4 males and one female). Two patients underwent laparotomy and a tumoral infiltration at the level of rectal–sigmoid and cecal appendix was found[11]. Four children with malakoplakia of the gastrointestinal tract were treated in Saudi Arabia between 1979 and 1983. In one patient malakoplakia was an incidental finding, while the remaining three patients presented with bloody diarrhea, recurrent fever and malnutrition. Colonoscopy revealed markedly inflamed and friable mucosa and pseudopolyps. They were treated with antibiotics[12]. Another case was a young girl who is presented from Pakistan, with rectal prolapse not responding to conservative therapy. Colonoscopy showed diffuse colitis with superficial ulcerations and pseudopolyps. Colon biopsies finally showed classical features of malakoplakia. In this case the conservative treatment failed and ultimately proctocoloctomy was performed[13]. Urinary tract including bladder, and colon were involved. She had presented with massive rectal bleeding associated with persistent urinary tract infection. Another observation in a 16 year-old girl with isolated bladder malakoplakia is reported by Steell et al. Ultrasound showed the bladder wall studded with multiple solid masses. Histopathology tests confirmed the changes as malakopladia[14]. Conclusion Malakoplakia is thought to be the result of abnormal macrophage function, often in patients with disrupted response to infection. Histological hallmark of the disease is the Michaelis-Gutmann body, an intracytoplasmic inclusion that arises in phagolysosomes which contains undigested bacterial fragments. Malaoplakia is found frequently, but not exclusively, in the bladder and colon. Colonoscopy and biopsy are the first modality requested for evaluation of chronic bloody diarrhea or hematochezia in children. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08016f1.jpg] |
| |||||||||

{kind=link}