 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 18, No. 3, Sept, 2008, pp. 222-228 Clinical Profile and Outcome in Children of Dengue Hemorrhagic Fever in North India Gurdeep S. Dhooria*1, MD, Pediatrician; Deepak Bhat1, MD, ediatrician; Harmesh S Bains1, MD, Pediatrician Department of Pediatrics, Dayanand Medical College, Ludhiana, Punjab, India Code Number: pe08035 Abstract Objective: The number of dengue fever (DF)/dengue hemorrhagic fever (DHF) cases reported in India has risen in recent years. This study was undertaken to evaluate clinical profile and outcome of children admitted with DHF/dengue shock syndrome (DSS), in the 2006 DHF epidemic in Ludhiana, Punjab. Key Words:Dengue hemorrhagic fever; Dengue shock syndrome; Epidemic; Mortality Introduction Dengue fever, the most important mosquito-borne viral disease, is endemic in more than 100 countries[1]. Dengue constitutes a major cause of pediatric morbidity and mortality in South East Asian countries[2]. Dengue fever (DF) has been reported from India over a long time, but dengue hemorrhagic fever (DHF) was first reported in 1963 from Calcutta city[3]. Since then several outbreaks of dengue fever have been reported from India with a major epidemic of dengue hemorrhagic fever that occurred in Delhi in 1996 when 10 252 cases and 423 deaths were reported[3]. The number of DF/DHF cases and deaths reported since the epidemic has been low till 2002 but again has risen since 2003. The case fatality has been above 1% for the last 10 years[3]. In India, dengue virus activity has been reported in many parts of the country with sudden epidemics over the last few years. Seasonal and cyclic epidemic pattern of dengue is a recerecent phenomenon Northern India[ 4-6]. The identification of dengue cases is by distinct clinical features but they can present with varied manifestations[7]. Manifestation in children and adults differ in many ways. In a study, children had higher proportion of DHF I (42.9%) cases, whereas 51% adults were of DHF II. Some clinical manifestations, such as petechiae, melena, headache, retro-orbital pain, joint pain, myalgia, nausea and vomiting were more common in adult patients[8]. Signs found commonly in children were epistaxis, oliguria, and liver enlargement. Hemoconcentration, thrombocytopenia, increased alanine aminotransferase, and longer prothrombin time were found to be higher in adults than in children[8]. Dengue remains a puzzling disease in many aspects, such as the virus-vector and host-virus relationship, and clinical expression variability[9]. This study was undertaken to evaluate clinical profile and outcome of children admitted with DHF/ Dengue Shock Syndrome(DSS), in the DHF epidemic in Ludhiana in 2006. Subjects & Methods This was a hospital based retrospective study. During the year 2005-06 dengue epidemic, 81 children with dengue hemorrhagic fever (DHF) were hospitalized in the Pediatric Department of Dayanand Medical College and Hospital, Ludhiana, India. An approval from the institution’s ethical committee was taken. Medical records of these 81 children were analyzed. The criteria used for diagnosing DHF included: an acute febrile illness of less than 10 days’ duration with purpuric spots or mucosal bleeding, hepatomegaly, and shock (any two), plus thrombocytopenia or raised hematocrit (any one). For the diagnosis of dengue shock syndrome (DSS), in addition to the previously mentioned criteria, the presence of hypotension or narrow pulse pressure was required. Thrombocytopenia was defined as platelet counts less than 100,000/cumm (part of case definition of DHF) and was further categorized, depending on severity as those with platelet count less than 50,000/cumm and with platelet count less than 20,000/ cumm. Of these 81 patients, 6 fulfilled the criteria for the diagnosis of DSS. All patients underwent a detailed clinical evaluation and relevant investigations. Disease severity was assessed according to the WHO grading system:
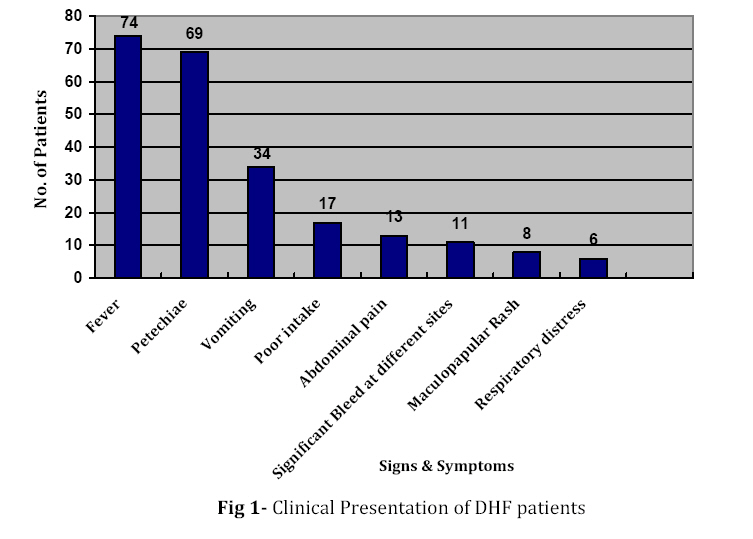
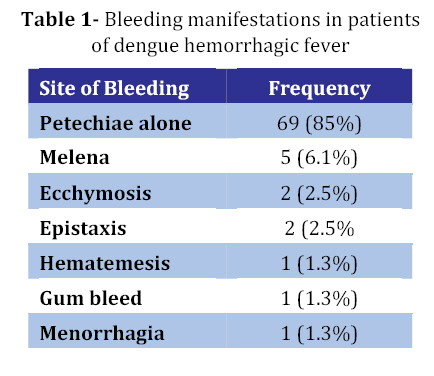
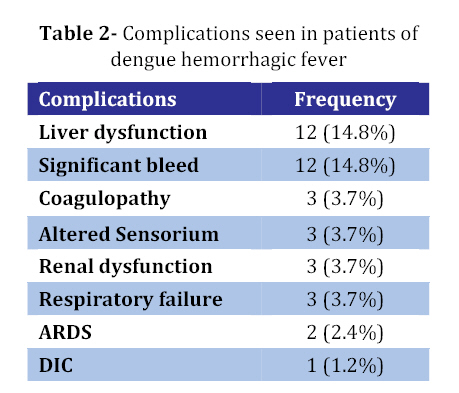
Grades III and IV DHF also referred to as DSS. All children were managed with fluids and blood products according to standard WHO guidelines. Severe cases of DHF were admitted in PICU. Hemoglobin, hematocrit, platelet count and total leukocyte count was done in all cases. Hemoconcentration was detected by serial hematocrit measurement. Platelet count was monitored as and when required in certain cases. Liver function test, chest X-ray and ultrasound abdomen was done in some patients. Other investigations like renal function tests, blood gas analysis, blood culture etc. were done according to clinical condition. Serological diagnosis was carried out with Panbio IgM Capture ELISA with antibody titres (>1.1) interpreted as positive-results. Patients in whom the serological tests were negative but presented with characteristic features of DHF or DSS, were included if no alternative bacterial or viral cause for the illness was identified. Findings Eighty one cases of DHF were admitted during the study period. Of these, 53 were males. Children between 10-15 years were most commonly afflicted (59%). Infants were the least affected sub-group with 3 cases (3.7%) all of which survived. The youngest child affected was 9 months old. The common symptoms seen were fever (91%), vomiting (41%), poor intake (21%), abdominal pain (16%) and significant bleeding (15%). The mean duration of fever was 5.08 days. Hepatomegaly was present in 60% of the cases (Fig. 1). While 85% of cases had petechiae alone, 12 patients (15%) had evidence of significant hemorrhagic manifestations such as ecchymosis and mucus membrane bleeds, upper or lower gastro-intestinal tract (GIT) bleeds and prolonged ooze from venepuncture sites (Table 1). Of these, 3 patients remained hypotensive, despite fluid resuscitation and inotropic support and had poor outcome. Ninety two percent of all children (65 patients) were in DHF grade II. Only 6 patients (7.4%) presented in DSS, with no patient presenting in DHF grade IV, of these six patients, 3 patients expired. The mean hematocrit at presentation was 35.5 (SD=3.92) gm%. The mean platelet count was 51,333 (SD=26,187)/cumm. Hematocrit more than 40% was seen in 27% of cases. All patients had platelet counts less than 100,000/cumm (part of case definition of DHF). Forty-one percent of cases had platelet count more than 50,000/cumm while 59% of cases had platelet count less than 50,000/cumm. Platelet counts was below 20,000/cumm in 14.8% of children. Disordered coagulation (prolongation of the prothrombin and/or partial thromboplastin time) was seen in 3 children (3.7%) and 1 child had disseminated intravascular coagulation (DIC). Hepatic dysfunction was seen in 14.8% children with greater than a three-fold elevation of hepatic transaminases. The highest value of transaminases seen was 3000IU/L (ALT) and 1500 IU/L (AST) in one child who also had coagulopathy and acute respiratory distress syndrome (ARDS) and died. Hyponatremia (<125 mEq/L) was seen in 5 cases of which 3 had poor outcome. Six patients presented with hypotension in the Emergency Room, fluid resuscitation was done in accordance with the WHO regimen. Three patients remained in shock despite fluid resuscitation, packed cell transfusions and inotropes but had poor outcome. Myocardial function and filling status could not be assessedby echocardiography in these patients due to financial constraints. Apart from shock, third spacing was manifest as pleural effusion in 9 children (11%). No patient had ascites. In addition to pleural effusion in 9 patients, 2 children fulfilled the criteria for ARDS, both presented with DSS and expired. Three children required assisted ventilation, 2 patients had ARDS. Of the 3 patients (3.7%) which presented with altered sensorium, 1 patient had persistent low Glasgow Coma Scale and seizures despite correction of shock. Dengue encephalopathy was suspected in view of normal metabolic profile and CSF examination. Brain imaging could not be done in this patient. Renal dysfunction was encountered in 3 children with a mean creatinine value of 1.5 mg/dl, none of whom underwent peritoneal dialysis, all of these children had poor outcome. The various complications seen in the series were as shown in Table 2. Co-infections were suspected in the presence of unusual clinical and/or laboratory features and were confirmed in 3 patients. Two children had septicemia and 1 patient had co-infection with enteric fever. All co- infections responded to appropriate drug and supportive therapy in addition to fluidresuscitation. Three out of 81 cases with DHF died resulting in a case fatality rate of 3.7%. Post-mortem examination could not be performed in any patient. Refractory shock and coagulopathy was present in all of these patients. In addition, 2 patients had ARDS and 1 patient had Encephalopathy. Discussion In this study of 81 cases of dengue hemorrhagic fever (DHF) most of the cases (91%) were of less than 6 yrs of age. Only 3.7% of cases were infants. In a study by Faridi et al, 76 % of all cases of DHF /DSSwere aged 6 years or more[10]. In a study by Anju et al, 45% cases presented with DHF/DSSat the age of 6 years or less of which 9% of cases were infants[11]. In our study, 92% of cases presented in Grade II and 7.4% cases presented in Grade III of WHO classification. No patient presented in Grade IV severity. Patients with Grade I disease did not require admission. In a study by Ratageri et al, dengue fever was present in 18%, DHF in 60% and DSS in 22% of cases[9]. In a study of 134 cases by Anju et al 67% of cases were of DHF whereas remaining 33% were of DSS[11]. In this study, common symptoms seen were fever (91%), vomiting (41%), poor intake (21%), abdominal pain(16%) and significant bleeding (15%). Hepatomegaly was seen in 60% of our cases. Ratageri et al reported fever (100%), vomiting (82%), abdominal pain (61%), restlessness (65%), headache (22%), and hepatomegaly (87%)[9].The mean duration of fever prior to admission was 5.47 days (2-12 days)[9] which was similar to our study. The most common bleeding manifestation was petechiae seen in 85% of cases. Significant bleeding was seen in the form of melena (6%), ecchymosis (2.5%) and epistaxis (2.5%). In a study by Ratageri et al, common bleeding manifestations were GI bleeding (22%) and petechiae (18%)[9]. Gastrointestinal tract was reported as the commonest site of bleeding (61%) in a study by Ahmed et al[13] as well as Rachel et al[12]. In our study, gastrointestinalbleeding in the form of melena and hematemesiswas seen in 7.4% of cases. Gastrointestinal bleeding is secondary to microvascular damage leading to increased permeability (particularly when platelet function is decreased) or actual disruption and local hemorrhage[14]. The main pathogenic feature of dengue is an increase in vascular permeability leading to loss of plasma from blood vessels, which causes hemoconcentration, low blood pressure and shock. This may also be accompanied by hemostatic abnormalities such as thrombocytopenia, vascular changes and coagulopathy[15]. A drop in platelet count to below 100,000/cumm and an increase of 20% or more in the hematocrit, both resulting from increased vascular permeability, are consistent findings. Other signs of plasma leakage include pleural effusion, ascites and hypoproteinemia. In the study the mean hematocrit at presentation was 35.5 gm%. Only 27% cases had hematocrit more than 40% and since pre-illness hematocrit was not known it was difficult to document hemoconcentration. These observations suggest that hemoconcentration may not be a good indicator for diagnosis and monitoring of fluid if pre-illness hematocrit is not known, particularly because there is a high prevalence of anemia in the population[13]. In the current study, all patients had platelet counts less than 100,000/cumm (part of case definition of DHF), while 59% of cases had platelet count less than 50,000/cumm. Twelve children had platelet counts below 20,000/cumm but only one child had evidence of spontaneous bleeding. Although thrombocytopenia was a constant finding, there was poor correlation between thrombocytopenia and bleeding diathesis. No correlation was found between platelet count and ecchymosis, indicating thereby that the abnormal platelet aggregation rather than reduction in absolute numbers was the cause of bleeding diathesis. In the study by Kamath et al, platelet counts less than 50,000/cumm were noted in 62.3%[16]. DHF patients with a platelet count less than 50,000/cumm were found to have a six-fold higher mortality than those with platelet counts more than 50,000/cumm[17]. In the present study, no deaths occurred in children with platelet counts greater than 50,000/cumm. Shivbalan et al found alanine transaminase (ALT), tender hepatomegaly, abdominal pain, abdominal distension and respiratory distress to be significant predictors for bleeding in dengue[18]. In our study, hepatic dysfunction was seen in 12 children (14.8%). It was noted thatpatients who did not survive had severe liver function abnormalities. Daniel et al suggested an association of abnormal aspartate transaminase (AST) with a worse outcome[12]. In our study, along with coagulopathy in the form of prolonged PT and PTT, respiratory distress was also associated with poor outcome. Dilutional hyponatremia and hypoproteinemia has been correlated with disease severity[19]. In our study, out of 5 patients with significant hyponatremia, 3 patients had poor outcome. Dengue infection can cause neurological manifestation ranging from non-specific symptoms to encephalitis and rarely Guillain-Barre Syndrome[20]. Apart from abnormal neurology secondary to cerebral hypoperfusion on account of shock other significant reasons for neurological presentations include cerebral edema, direct neurotropic effect of dengue virus resulting in encephalitis/ encephalopathy, or secondary to hepatic dysfunction and metabolic derangements such as hypoglycemia and hyponatremia[21-24]. Encephalopathy is known to occur in 0.5%of patients with DHF[25]. Malavige et al reported acute liver failure (73%), electrolyte imbalances (80%) and shock (40%) as factors contributing to encephalopathy[26]. In our study, of the 3 patients (3.7%) which presented with altered sensorium, 1 patient had persistent low GSC and seizures inspite of correction of shock. Dengue encephalopathy was suspected in view of normal metabolic profile and CSF examination. Two of our patients had ARDS, both of which expired. Dengue associated ARDS is associated with a high mortality[27]. Mortality in the present study was 3.7%. All patients who expired belonged to DSS. In the study by Anju et al overall mortality seen was 6%[11], compared to 3% by Ahmed et al[13]. This could be due to delay in recognition of epidemic in previous years or delay in seeking medical attention. Case fatality rate (CFR) of the SEAR countries in 2006 is less than 1%. India, Indonesia, Bhutan and Nepal still have case fatality rates above 1%[28].Early diagnosis and improved case management of DHF/DSS is required to bring down CFR to below 1%. Conclusion Common age group afflicted in our study was 10-15 years. Majority (92%) of the patients presented in Grade II DHF. Respiratory distress and coagulopathy were the bad prognostic factors. Increased awareness, better transport facilities and case management according to the WHO guidelines, is needed to further reduce mortality of DHF/DSS cases. Acknowledgement We are thankful to Dr Daljit Singh, Principal & Professor (Pediatrics), for his constant guidance and moral support. GSD– concept, design, analysis and interpretation of data and drafting of the article; DB- acquisition, analysis of data, also helped in prepration of manuscript, HSB-, revising it critically for important intellectual content and final approval and will act as guarantor for the study. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08035t2.jpg] [pe08035t1.jpg] [pe08035f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}