 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
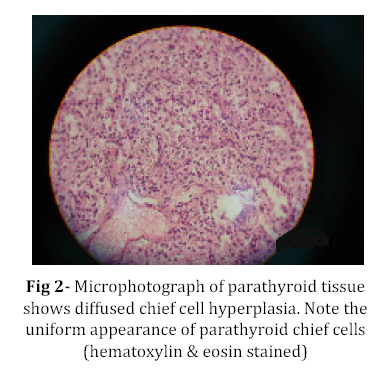
Iranian Journal of Pediatrics, Vol. 18, No. 3, Sept, 2008, pp. 277-280 Severe Neonatal Hypercalcemia due to Primary Hyperparathyroidism; A Case Report Siamak Shiva*1, MD, Pediatric Endocrinologist; Alireza Nikzad1, MD, General Physician; Saeid Aslanabadi2, Pediatric Surgeon; Vahid Montazeri3, MD, Thoracic surgeon; Mohammad-Reza Nikzad1, MD, General Physician 1. Department of Pediatrics, Tabriz University of Medical Sciences, IR Iran Code Number: pe08044 Abstract Background:Neonatal primary hyperparathyroidism (NPHP) is a rare disease characterized by marked hypercalcemia, diffuse parathyroid hyperplasia and skeletal demineralization. These patients have symptoms of chronic hypercalcemia such as failure to thrive, irritability, abdominal pain and anorexia. It is often fatal unless parathyroidectomy is performed.Treatment with drugs usually is inadequate and often results in chronic hypercalcemia and death. Key Words: Primary hyperparathyroidism; Neonate; Parathyroidectomy; Autotransplantation Introduction Neonatal primary hyperparathyroidism (NPHP) is a rare disease that presents in the first 6 months of life[1]. It is almost invariably fatal unless a prompt diagnosis is made and urgent surgical intervention instituted[2]. It is associated with hypotonia, respiratory distress, irritability, lethargy, failure to thrive, constipation and severe hypercalcemia with elevated parathyroid hormone (PTH) levels[1]. Radiographs show severe bone demineralization[1,3]. The etiology is genetic[4] and results from inactivating mutation of calcium sensing receptor gene, in which the inhibitory effect of extracellular calcium on the secretion of PTH by chief cell is absent[1]. All reported cases of NPHP have been due to parathyroid chief cell hyperplasia[1-6]. Surgical treatment with subtotal parathyroidectomy, total parathyroidectomy or total parathyroidectomy with autotransplantation, is preferred modality. The mortality rate with this modality is 24%[7]. About 50 neonates with NPHP have been reported and it has been suggested as a possible contributor to a small number of cases of the Sudden Infant Death Syndrome[2,4]. The authors report on a case presenting in a male neonate, review the world literature and discuss the clinical manifestations, investigators' findings and the management options available. Case Presentation A 10-day-old 2.9 kg male newborn was hospitalized for anorexia, poor feeding, cyanosis, hypotonia, lethargy and severe dehydration. He was a full term baby at birth weighing 3400 grams and his parents were related (cousins).Despite rehydration, he had hypercalcemia with Ca concentration of 18.2 mg/dl (normal, 8.6 to 10.3). Other laboratory findings were serum PTH level of 996 pg/ml (Normal, 7 to 82), phosphorus level of 1.6 mg/dl (Normal, 4 to 6.5) and alkaline phosphatase level of 1322 IU/L (Normal, 180 to 1200). Urine Ca excretion was 12 mg/kg/d. Evaluation of mother for serum levels of Ca, P and PTH showed normal values.With vigorous medical management using saline diuresis, furosemide, hydrocortisone and intravenous pamidronate 1mg/kg/d for 3 days, serum Ca level remained between 13-15 mg/dl.Full skeletal survey revealed severe and generalized osteopenia. Bone density was diffusely decreased and multiple regions of pathologic fractures in proximal and distal parts of femur, humerus and ribs along with lung calcification were seen (Fig 1). Ultrasound revealed medullary nephrocalcinosis; echocardiography was normal. 99M-TC-sestaMIBI scan showed homogeneous uptake of the radiotracer in parathyroid glands with no evidence of parathyroid adenoma.Combination of clinical, laboratory and radiological findings were consistent with the diagnosis of NPHP. Since patient did not respond to the medical therapy and his symptoms persisted, surgical approach was considered. We performed total parathyroidectomy with autotransplantation. After removing all 4 parathyroid glands, a portion of a gland was autotransplanted in sternocleidomastoid muscle. Because of hypocalcemia (serum Ca 7.5 mg/dl) we started calcium supplementation and vitamin D therapy during the second day after surgery. Two months after surgery patient was eucalcemic and had no need for vitamin D supplementation. Histological examination of parathyroid glands revealed diffuse chief cell hyperplasia (Fig 2). Discussion Neonatal primary hyperparathyroidism (NPHP) is a rare disease, which is often fatal. This condition results from chief cell hyperplasia and excessive secretion of PTH[3-6]. Usually symptoms manifest in the first days after birth[4]. Symptoms include poor feeding, irritability, constipation, polyuria, hypotonia, respiratory distress and bone abnormality such as osteopenia, subperiosteal bone resorption, pathologic fracture and failure to thrive almost in all cases[4,5]. NPHP is characterized by marked hypercalcemia, hypophosphatemia, hyper-phosphaturia, hypercalciuria and elevated PTH level[3,4]. In differential diagnosis other causes of hypercalcemia should be considered including: iatrogenic hypercalcemia (calcium salts), idiopathic infantile hypercalcemia, Williams syndrome, vitamin D intoxication and familial hypocalciuric hypercalcemia (FHH). FHH manifests with elevated serum levels of calcium and magnesium. Patients with this disease have normal phosphate and calcitriol levels with no hypercalciuria. PTH level could be normal or mildly elevated[3-5]. Hypercalcemia lasts life-long; patients have no other problems[5]. Most patients do not require any treatment. In contrast, NPHP can be life-threatening if left untreated[1]. Mutations in the calcium-sensing receptor (CASR) gene which lead to loss of normal function of these receptors can be seen in both FHH and NPHP. Activation of CASR by extracellular calcium inhibits secretion of PTH by the chief cells[1,9]. In NPHP, medical therapy is inadequate and surgical modality should be considered[3-5]. This intervention must be undertaken immediately to avoid death or irreversible long term complications such as nephrocalcinosis, cardiac abnormalities, bone resorption, or central nervous system alterations[4]. As in our case many other reports show that the treatment of choice is total parathyro-idectomy with autotransplantation[4,10-13]. Without parathyroidectomy, affected infants will usually die by the age of three months[10]. Medical therapy without surgical intervention has a mortality rate of 70% to 87% and severe long term complications in the survivors[4]. Ross et al reported that seven of eight patients treated medically for primary hyperparathyroidism died in infancy, with a mortality rate of 87.5% and the mortality rate among patients treated surgically was reduced to 24%[7]. Meeran et al reported a case with NPHP who survived without parathyroidectomy to an age of nine months, in whom no fractures were observed and the hypercalcaemia became masked by vitamin D deficiency[10]. These patients are critically ill at presentation and initial therapy with hydration, furosemide, steroids, and intravenous pamidronate are not enough to control hypercalcemia completely[11,14]. Despite the intensive medical therapy it was not easy to prepare the severely ill patient for parathyroidectomy. Three possible surgical procedures for these patients are: total parathyroidectomy, subtotal parathyroidectomy or total parathyroidectomy with autotransplantation. Total parathyroidectomy leads to hypoparathyroidism with a life-long need to calcium and vitamin D supplementation. In total parathyroidectomy with autotransplanttation all 4 parathyroid glands are removed and a small portion of a gland is implanted into intramuscular pockets[1-5,8]. Excellent results obtained in our patient demonstrate that total parathyroidectomy with autotransplantation could successfully regulate calcium homeostasis in severe primary hyperparathyroidism. However, we should not forget that hypercalcemia may recur in this patient in the future. Conclusion Although NPHP is a rare disease, it must be considered for differential diagnosis in neonates with severe hypercalcemia. Early diagnosis and total parathyroidectomy with autotransplantation can be life-saving. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08044f1.jpg] [pe08044f2.jpg] |
| |||||||||

{kind=link}
{kind=link}