 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
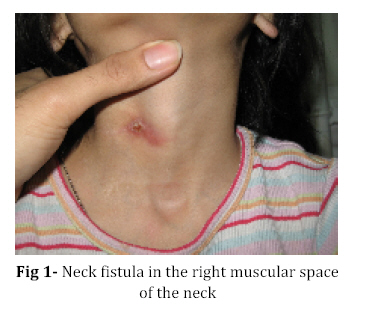
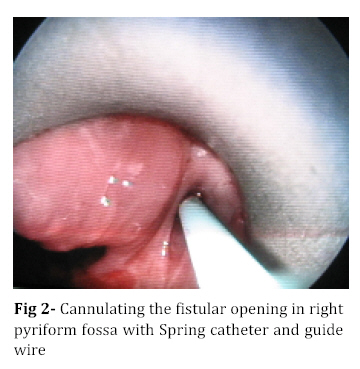
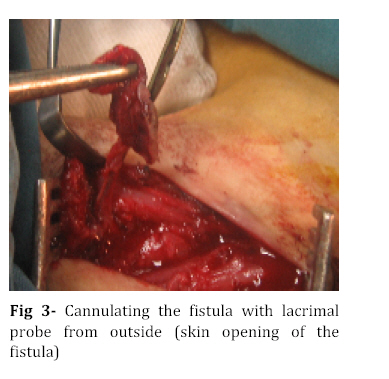
Iranian Journal of Pediatrics, Vol. 18, No. 3, Sept, 2008, pp. 285-289 Reporting a Right Sided 4th Branchial Anomaly; Case Report and Reporting the Technical Issues Mohammadtaghi Khorsandi Ashtiani1, MD, Otorhinolaryngologist; Nasrin Yazdani1, MD, Otorhinolaryngologist; Shahin Bastaninejad*1, MD, Resident in Otorhinolaryngology; Mohammadhossein Dadgarnia2, MD, Otorhinolaryngologist 1. Department of Otorhinolaryngology, Tehran University of Medical Sciences, IR Iran Code Number: pe08046 Abstarct Background:Fourth branchial pouch anomaly (4BPA) is a rare condition that often presents an extreme diagnostic and therapeutic challenge. It usually causes recurrent left thyroid or perithyroid tissue inflammation, but it can be situated in the right side too. Key Words:Fourth branchial anomaly; Pyriform sinus fistula; Neck fistula; Recurrent thyroid abscess Introduction Third and fourth branchial cleft anomalies may result in cyst and/or abscess in the thyroid or perithyroid tissue[1]. These are challenging diagnostic and therapeutic entities in the head and neck surgical field. The third and fourth branchial pouches are connected to the pharynx by the pharyngobranchial duct. Failure of this duct to degenerate in the seventh week of gestation leads to a persistent communication with the pyriform fossa of the hypopharynx[2]. There is a convoluted theoretical course for 4th branchial pouch anomaly (4BPA), this tract originates within the pyriform fossa and follows a convoluted course exiting the larynx near the cricothyroid joint and coursing between the superior and recurrent laryngeal nerves. On the left side, this tract follows the tracheoesophageal groove to the level of the aorta; on the right, it descends only to the level of the subclavian artery. In both cases, the tract then traverses beneath its respective vessel, ascends posterior to the common carotid artery, passes above the hypoglossal nerve, and exits the neck anteriorly at the sternocleidomastoid muscle. Acomplete fourth arch fistula has never been reported, and anomalies of both the third and fourth branchial pouch begin in the pyriform fossa[2]. Differentiating 3rd branchial anomaly and 4BPA is often the purview of the operating table: if the course of the sinus is found cephalad to the superior laryngeal nerve and cricothyroid muscle, the disease is of the third branchial apparatus. If caudal, the fourth branchial pouch is implicated[2]. Definitive treatment of 4BPA is surgical resection. However, curative surgery should only be attempted in the absence of acute infection. As a result, patients presenting with infection should be treated with aggressive antibiotics, and elective resection of the branchial cleft sinus is delayed for several weeks afterward[2]. Barium swallow, if used in the quiescent stage of the disease, has 80% sensitivity for demonstrating the anomalous tract[3]. Incision and drainage and antibiotic treatment may be used as temporizing measures before proceeding with the definitive surgery[3]. Case Presentation A nine-year-old girl was referred to our tertiary otolaryngology and head and neck surgery center - Amiralam Hospital - for evaluation of recurrent right muscular space mass and fistulathat was unresponsive to any medical or surgical procedures (Fig 1). Her problem started about two years ago with two episodes of abscess formation in her right muscular space of the neck that was managed in pediatric departments with intravenous antibiotics and repeated aspirations. Six months after the last episode of neck swelling, she was admitted in an otolaryngology center. There her neck was explored and right lobectomy of the thyroid gland was performed. She was all right for about four months, but again her neck swelling recurred in the right muscular triangle. Two months after that, we admit her in our hospital. Here we seek for infectious causes, (including tuberculosis, actinomyces, and fungi) all being negative. We decided to proceed with the second surgical approach. The neck mass was getting indurate and enlarged day by day before the second operation, three days before the operation a fistula appeared on the top of the bulging. Before the second operation (the first operation in our institute), we perform rigid pharyngoscopy in general anesthesia, which shows no opening in the pyriform fossa, so we decide to perform only a simple incision and drainage, before proceeding with this operation. We cannulate the fistula and it guides to a probable tract. Neck exploration and complete resection of the lesion after dissecting the cervical plans that were hardened by acute inflammation and massive fibrosis due to the previous operation, we seek any tract in all directions but we couldn’t find any, also we remove all inflammatory tissues. The final pathology report indicates “chronic inflammation”. Unfortunately four months later, the neck mass recurred again and the fistula begun to drain. After several weeks the neck mass resolved completely but neck fistula persists (Fig 1). The patient had no cooperation for a close follow up for several months, but finally, eight months after establishment of the neck fistula, her mother brought her and said that, sometimeswhen she drinks, it comes through the neck fistula. So, a third operation was planned. Inflammatory and neoplastic lesions had been already ruled out in the past, so the only probability was an uncommon congenital lesion situated on the right muscular space. The lesion was in a quiescent stage, without any swelling or infectious signs. We performed a modified barium swallow radiography and then (for tracing barium in the hypopharyngeal lumen) an axial neck computed tomographic scan. Unfortunately these procedures added nothing to our knowledge about her neck fistula. On the operating table, first we performed again a rigid pharyngoscopy, this procedure revealed the fistular opening which was situated in the right pyriform fossa. Regarding the existing literature, we cannulated it with a Spring catheter and its flexible guide wire (it is a kind of vascular catheter), then we begun to operate on the neck (Fig 2). The operation field and cervical plans were complicated with massive fibrosis (due to the previous operations and chronic inflammation), so, in the present situation we didn’t decide to find and dissect recurrent laryngeal nerve. In the proceeding steps of dissecting the fistula from the surrounding tissues, we found that Spring catheter was curved and directed toward the pyriform apex mucosa, where it made a dangerous mucosal tearing, so, we removed it and cannulated the fistula with a lacrimal probe from outside and checked its internal position with rigid laryngoscope, indeed lacrimal probe was inserted into the pyriform opening of the fistula from outside (Fig 3). We continued dissection till the pyriform area was approached, where we ligated and cut the tract entirely, and repaired the mucosal tearing that was induced by Spring catheter with meticulous submucosal suturing. The tract direction to the pyriform sinus was beneath and caudal to the cricothyroid muscle, so, we assume its origin to be a remnant of pharyngobranchial duct of the 4th branchial pouch anomaly. Fortunately patient has no vocal cord paralysis and pathology confirmed the existence of branchial duct in the tissue specimen. One year after the final operation there is no evidence of recurrence. Discussion Symptoms on the right side of the neck do not exclude the diagnosis of a 4BPA[4]. Direct pharyngoscopy allowed confirmation of the diagnosis in our patient and also permitted catheterization of the tract with the Spring guidewire and checking the correct position of lacrimal probe that was inserted externally, which helped us in surgical localization and subsequent neck dissection. We performed direct pharyngoscopy in the active phase of infection previously, it revealed nothing to us, so, it’s logical to postpone any diagnostic and main surgical efforts, after complete resolution of infection.In literature it is recommended to cannulate the pyriform opening with a lacrimal probe, Fogarty catheter, Spring catheter and[4] also it is recommended that if the entire tract cannot be cannulated, palpation of the catheter in the most proximal portion will assist with identifying and ligating the tract[5], but to our experience, it may be hazardous, so, when there is another orifice in a safer place such as skin it is amenable to try to cannulate this opening at first, because of more convenience, easier accessibility and less traumatizing potentials. Identification and dissection of the recurrent laryngeal nerve is a controversial subject, some authors advocate its exposure in all cases in such a manner that, they may terminate operation if this is impossible[2]. We did not dissect the recurrent laryngeal nerve, because of the extensive fibrosis in the dissection field. Postoperatively our patient was well, without any vocal cords problem. It is of utmost importance that the involved thyroid parenchyma be resected during the operation and the tract be ligated at the level of the pyriform sinus to minimize the risk of recurrence[3]. In our case thyroid lobectomy was performed previously (in the first operation) and also we ligated the tract at the pyriform sinus level as well. Regardless of literature, Barium swallow study and neck CT-scan with modified valsalva maneuver yielded no additional information about the final diagnosis. Conclusion A recurrent left or right lower neck abscess in the thyroid or perithyroid tissues, that recurs, in spite of appropriate antibiotics and surgical drainage, should raise the suspicion of 4BPA and must be managed and investigated mainly with conservative measures or simple incision and drainage procedure, till the quiescent stage of the infectious process, when thorough diagnostic measures can be performed and the final operation timing and strategy planned. This must include rigid pharyngoscopy that will allow confirmation of the diagnosis and permit catheterization of the tract which is crucial for complete tract removal. In patients with both skin fistula and pyriform sinus opening, external cannulation is more convenient and less traumatizing than internal catheterization. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08046f2.jpg] [pe08046f1.jpg] [pe08046f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}