 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
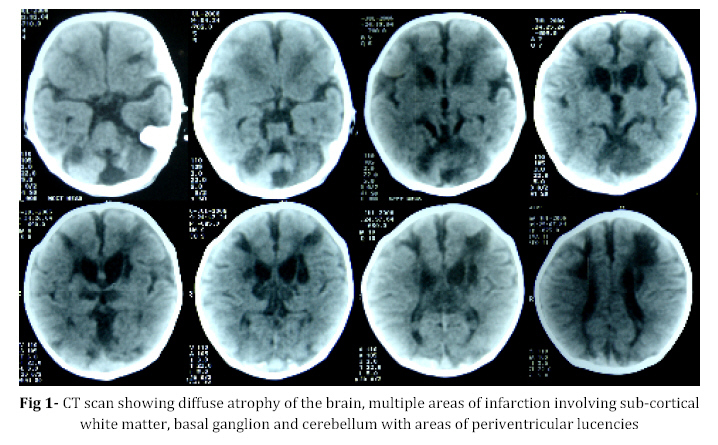
Iranian Journal of Pediatrics, Vol. 18, No. 3, Sept, 2008, pp. 289-290 Letter to Editor Antenatal Hypoxic-ischemic Insult Amit Agrawal*1, MD, MCh, Neurosurgeon Department of Surgery, Datta Meghe Institute of Medical Sciences, Sawangi, Wardha, India Code Number: pe08047 Newborn hypoxic-ischemic encephalopathy is an important clinical problem associated with considerable morbidity and mortality. Birth prevalence ranges from 1.8 to 7.7 per 1000 term live births[1,2,3]. This 27 days male child presented with small size of head, not accepting feeds and listlessness. He was born at full term at home with normal vaginal delivery. At 6th month of gestation mother had fever and took some medication for the same however details were not available. On examination head circumference was 30 cm and coronal suture was fused. Child was dull and less active. CT scan showed diffuse brain atrophy and multiple infarctions (Fig 1). It is now widely recognized that the majority of cases of term neonatal encephalopathy are related to hypoxic-ischemic brain injury that occurs in utero from a variety of intrapartum conditions[4]. Thyroid disease, severe pre-eclampsia, moderate or severe vaginal bleeding in pregnancy and a documented medical attendance for a presumed viral infection are all associated with an increased risk[4]. The role of perinatal infection is of considerable aetiological interest in neurological dysfunction in preterm 5 and term6 infants. In addition to the well known viral teratogens (rubella, cytomegalovirus) other viruses may be teratogenic or other mechanisms may operate such as hyperthermia[7], inflammatory mediators, or other pathophysiological responses[8]. Hypoxia-ischemia results in selective damage to different brain structures depending on the developmental stage at which it occurs[9]. Hypoxia-ischemia in the preterm human (gestational week 23-32) causes damage to subcortical developing white matter, a condition known as periventricular leukomalacia (PVL)[10]. Developmental immaturity of the cerebral vasculature is thought to account for this characteristic subcortical distribution[11]. Hypoxia-ischemia in the preterm infant disrupts normal development and results in significant cerebral injury. Hypoxic-ischemic brain injury results in cerebral palsy, mental retardation, or learning disabilities in surviving children[12]. Neurological disability is observed in 51% of premature infants (GW<25 weeks) examined at 30 months of age[13] and persists into adulthood[14]. Deficits are found in motor, perceptual, and cognitive systems[10]. In order to optimize pre-natal, perinatal and neonatal care, it is necessary to detect factors responsible for brain damage and obtain information about their timing[15]. Knowledge of the timing of asphyxia, infections and circulatory abnormalities would enable obstetricians and neonatologists to improve prevention in pre-term and full-term neonates[15]. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08047f1.jpg] |
| |||||||||

{kind=link}