 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
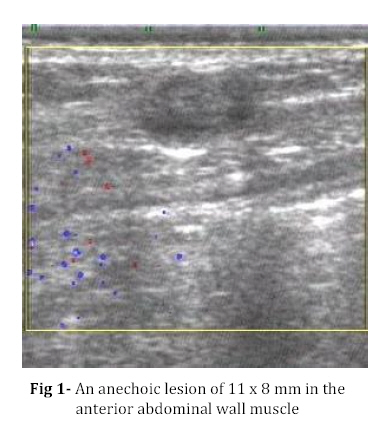
Iranian Journal of Pediatrics, Vol. 18, No. 3, Sept, 2008, pp. 291-292 A Rare Cause of Solitary Abdominal Wall Lesion Rizwan Ahmad Khan*1, MS, MCh; Pediatric Surgeon; Shagufta Wahab2, MD, Radiodiagnosis; Rajendra Singh Chana3, MS, MCh, Pediatric Surgeon 1. Department of Surgery, JNMCH, AMU, Aligarh, India Code Number: pe08048 A 7-year-old male child was brought to outpatient department by his mother with a complaint of painless nodule on the right side of the abdomen below the costal margin. Otherwise, the child was in good general health and had no other complaints. There was no history of trauma in the past. On inspection there was no evidence of swelling and it was only on very careful palpation a nodule of approximately 1.0 cm in diameter, which was freely movable, was felt in the right subcostal region. The overlying skin was normal. An FNAC was performed and it revealed a background of polymorphonuclear infiltrate rich in eosinophils and a typical wavy outer larval membrane with a stroma containing multiple ovid nuclei. An ultrasound of the exact region was obtained (Fig 1). Ultrasound image of the region showing an anechoic lesion of 11 x 8 mm in the anterior abdominal wall muscle (internal oblique) with its long axis being parallel to the muscle fibers. - What is the diagnosis? Solitary Abdominal Wall Cysticercosis Discussion Cysticercosis is a parasitic infection caused by Cysticercus cellulosae, the larval form of Taenia solium where as the infestation of human intestine with adult tapeworms is known as taeniasis. Humans are the only definitive host while both humans and pigs can act as intermediate hosts. The mode of transmission is feco-oral, the most common being the consumption of raw or undercookedbeef or pork, water, or vegetables contaminated with Taenia eggs[1]. The skeletal muscle, subcutaneous tissue, the eyes and CNS are the most frequently affected tissues. Other reported sites are heart, lungs, peritoneum, kidney, liver, and pancreas. Children are commonly affected because of increased chances of fomite infection[2]. The larvae get established in the tissues as fluid-filled cysts thereby evading the immune response of the host. The intramuscular and subcutaneous cysticercosis is seen most commonly over the arms and chest and is characterized by multiple, mobile, firm, subcutaneous nodules with normal overlying skin. The nodules vary in size from 1 to 2 cm and are usually asymptomatic. It may be painful in about 20% of the patients and there are chances of abscess formation as well[3]. The differential diagnosis includes lipomas, epidermoid cysts, neuroma, neurofibromas, pseudoganglia, sarcoma, myxoma or tuberculous lymphadenitis. Solitary muscular and soft tissue cysticercal involvement is a rare disease per se and it has been used as a marker of neurocysticercosis. Therefore, central nervous system or ocular involvement should be ruled out if systemic involvement is suspected[6]. Immunodiagnosis by enzyme-linked immuno-blot assay is more accurate than ELISA but sensitivity is low when parasite burden is low in solitary intramuscular or subcutaneous lesions[4]. The well established criteria on fine-needle cytology help to confirm the diagnosis of a subcutaneous cysticercosis nodule with the essential one being identification of parasitic fragments[5]. Other criteria include recognition of the tegument of the parasite which appears as rounded wavy folds and scolex with hooklets with hyaline membrane surrounding it. The inflammatory reaction consists mainly of eosinophils with varying proportions of other polymorphs and epithelioid cells and giant cells[5]. Radiological modalities, like MRI can also sometime show characteristic appearance of solitary cysticercosis and a scolex within. On ultrasonography the cyst can be seen as a clear anechoic structure with well-defined smooth walls. Sometimes, scolices can be easily appreciated on ultrasound than on MR images[6]. Early diagnosis helps to initiate appropriate therapy with cestocidal drugs, like pranziquantel or albendazol. Some authors are of the view that the anticysticercal treatment is unnecessary in asymptomatic cases while others recommend simultaneous use of steroids as well to prevent the adverse reactions. It has been observed that most of the nodules disappear months after the initiation of the treatment. Surgical excision can be considered for solitary or a few lesions as a definitive and cosmetic treatment[3]. The taeniasis-cysticercosis complex poses a difficult public health problem in poor countries particularly in parts of Asia and Africa and a disease prevention program involving proper sewage disposal, consumption of filtered or boiled water, preparation of well washed vegetables and beef before consumption is recommended. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08048f1.jpg] |
| |||||||||

{kind=link}