 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 18, No. 4, Dec, 2008, pp. 309-314 Multi Drug Resistant Tuberculous Meningitis in Pediatric Age Group Chander Prakash Baveja*1 , MBBS, MD; Vidyanidhi Gumma1 , MSc; Manisha Jain1 , MBBS, MD; Monica Chaudhary2 , MBBS,MD; Bibek Talukdar3 , MBBS, MD; Vinay Kumar Sharma4 , MBBS, MD 1. Department of Microbiology, Maulana Azad Medical College, Delhi, India * Correspondence author; Address: Department of Microbiology, Maulana Azad Medical College, BSZ Marg, New Delhi -110002, India E-mail: bavejac@indiatimes.com Received: 03/03/08; Revised: 13/06/08; Accepted: 10/08/08 Code Number: pe08050 Abstract Objective: Past decade has seen increase in cases of tuberculous meningitis (TBM) and
multidrug resistance in such cases. The mortality rate for a mismanaged TBM is very high
which increases manifold in presence of associated complicating factors. The present study was
thus planned to evaluate the prevalence of MDR-TBM and look for associated complicating
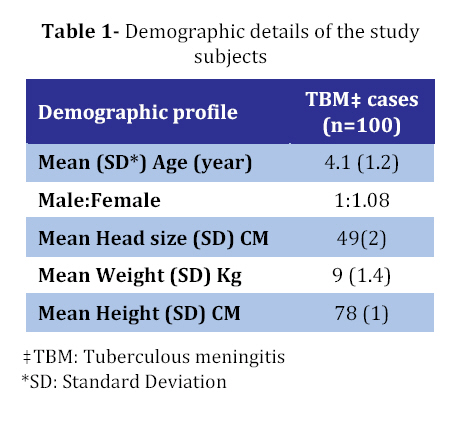
factors and carry out drug sensitivity pattern in all culture positive isolates. Key Words: Cerebrospinal fluid; Multidrug resistance drug; Tuberculous meningitis; BACTEC; Children Introduction Tuberculous meningitis (TBM) is one of the most severe manifestations of extra pulmonary tuberculosis (TB)[1,2]. The relative incidence of TBM has been reported to be around 7-12% of all cases of tuberculosis and it is relatively high during first five years of life[3]. From India it was seen in a previous study that 16.46% of deaths in pediatric wardswere due to tuberculosis ofvarious types and TBM accounted for around 56% of these cases[4]. There is paucity of literature regarding the prevalence of bacteriologically confirmed TBM worldwide and specially from India. But in a recent study from India it was seen that TBM still remains amajor cause of death and of neurological disabilities[5]. In the era of Human Immunodeficiency Virus (HIV) infection TBM has acquired added significance specially the prevalence of multidrug resistance has rose further complicating the ongoing epidemic of HIV[6]. Factors contributing to high mortality in case of TBM includes disseminated TB, HIV infection, delay in diagnosis and treatment and absence of standardized protocols for the management of multi drug resistance TBM (MDR-TBM)[7]. Case fatality in cases of untreated TBM is almost 100% and delay in initiating treatment may leave permanent sequelae[2,7]. In view of the manifold increased mortality as a result of delay in diagnosing MDR-TBM there is only a little margin for error. Anti tubercular treatment (ATT) is started on the presumptive diagnosis of TBM based on clinical presentation, biochemical and cytological evaluation of CSF, radiological investigations and the evidence of current or past tuberculosis. Clinical response to ATT also has been included as one of the criteria to presumptively diagnose TBM[8]. But recently few reports of multi drug resistance in TBM have been documented though limited to few case reports and only single case series[9,10,11]. There is paucity of data regarding the prevalence of definitive cases of TBM from India and multidrug resistance in such cases, hence the objective of the present study was to evaluate the prevalence of bacteriologically confirmed TBM and to look for multidrug resistance; other associated factors like HIV infection in such cases to help the clinicians about the newer challenges in the management of such patients. Subjects & Methods This was a hospital based prospective laboratory oriented observational study conducted at the Mycobacteriology laboratory, Maulana Azad Medical College and Department of Pediatrics at Lok Nayak Hospital Delhi, India from 2004 -2005. Selection criteria: The study group included children between 6 months to 12 years recruited into the study after an informed consent was obtained from their parents/guardians. They were presumptively identified as TBM on the basis of clinical suspicion by a set of diagnostic criteria as follows.
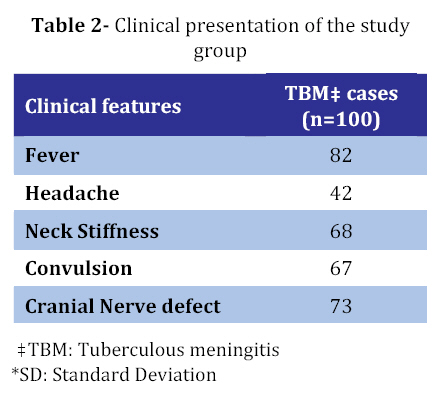
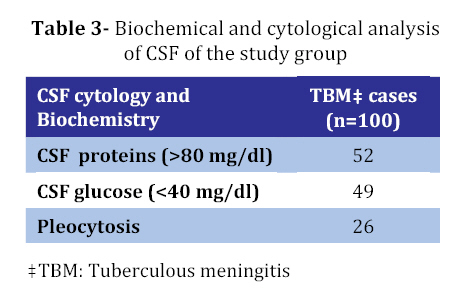
All the children who satisfied the clinical criteria with any one of the non-clinical criteria were initially labeled as presumptive TBM and were started on antitubercular treatment. Definitive diagnosis of TBM was made in patients by isolation of the tubercle bacilli from CSF either by direct microscopic examination or Mycobacterial culture. Exclusion criteria: Patients showing confirmatory evidence of alternative diagnosis during course of their treatment were excluded from study. A complete physical examination including a thorough neurological examination was undertaken to detect the common features of TBM. Lumbar puncture was performed in the study patients using all aseptic precautions and CSF was collected and aliquoted in appropriate specimen bottles for various investigations. Laboratory investigations: One ml of CSF was collected in a fluoride bottle for the estimation of glucose and protein levels. The sample was also sent for cytological evaluation. Differential cell count was performed on Giemsa stained smear. Routine bacteriological culture was performed as per standard protocols. For mycobacterial examination, the CSF was processed with great care being taken to avoid contamination or spillage. Direct microscopy: CSF was centrifuged at 3000g×15 min. The sediment was used for the preparation of smear and for culture. Approximately 20 µl of the sample was taken and was spread in an area of 2-3 cm. The smear was air dried and then heat fixed. It was then stained with Ziehl-Neelsen (ZN) stain and examined under microscope (×100). All the slides were examined by three independent examiners to ensure the accuracy. At least 300-500 oil immersion fields were screened before declaring it as negative. Culture: Centrifuged deposit of CSF was also inoculated on two bottles of Lowenstein- Jensen (LJ) culture media and BACTEC 12 B vial medium. These inoculated media were incubated at 37oC for up to 8 weeks. Cultures were examined first after 4 days and thereafter weekly till 8 weeks in LJ medium and in BACTEC 12 B vial medium, reading was taken according to manufacturer’s instruction. Positive growth on LJ culture medium was identified by typical colony morphology and was confirmed by performing a ZN staining. Positive Growth Index (GI) in BACTEC 12 B vial medium was also confirmed by ZN staining. Drug sensitivity by BACTEC method: Drug sensitivity was carried out by BACTEC 460 TB system according to manufacturer’s directions. Following concentrations were used: Streptomycin (STR) 2.0 mg/mL, Isoniazid (INH) 0.1 mg/mL, Rifampicin (RIF) 2.0 mg/mL, Ethambutol (EMB) 2.5 mg/mL. The four first line drugs were reconstituted in reconstitution fluid (RF). O.1 mL of the appropriate drug solution was injected into labeled 12B vials which resulted into the desired concentration of a drug in the medium. This was followed by inoculation of 0.1 mL of bacterial suspension from a positive 12B vial with a GI 500-800. For control, the bacterial inoculum was diluted 1:100 before inoculation. The inoculated 12B vials were incubated and read daily till the GI of the control reached >30. If the change in the GI (∆ GI) of the vial containing drug reaches more than 1% change in the GI of the control (∆ GI) or if the GI of the vial containing drug is more than the GI of control it is taken as resistance to this drug. If the GI of drug vial is less than the GI of the control it is taken as susceptible. Findings The mean age of the study group was 4 (SD=1.2) years. Males comprised 48% whereas females comprised 52% of the study population (Table 1). Most of the patients on admission presented with fever whereas other common complaints were neck stiffness, convulsion and headache (Table 2). On gross examination most of the CSF samples were clear with turbidity being present in only 8 (8 %) of the CSF samples. A clot was detected in standing CSF in only 5 samples. CSF studies: The biochemical analysis of the CSF sample revealed features consistent with tuberculosis meningitis (elevated CSF protein and reduced glucose levels) in almost 50% of the study subjects (Table 3). Among the definitive cases of TBM isolation of Mycobacterium tuberculosis from CSF through various methods was as follows: ZN Smear: The sensitivity of direct examination was very low being positive in only 2 patients. These two CSF samples were also positive for LJ culture and BACTEC culture. LJ Culture: The conventionally performed LJ culture gave positive results in 6 patients only. All these 6 patients were also positive on BACTEC culture. CSF BACTEC Culture and Drug Sensitivity: The yield from this method was 22 %. All these 22 positive growths were identified as Mycobacterium tuberculosis. Out of these 22 samples, 18 samples (81.8%) were sensitive to all the four drugs (RIF, STR, INH and EMB) whereas multi drug resistance could be detected in 4 (18.2%) samples. Two cases were resistant to RIF and INH, one case was resistant to RIF, INH, EMB whereas one case was resistant to all these four drugs.On further analysis of associated factors with multidrug resistance it was seen that one (25%) sample out of these 4 was HIV positive. Amongst the remaining three patients, one patient also gave previous history of anti- tubercular treatment. Follow up data was available for 19 of the 22 definitive cases of TBM, 3 of the 4 MDR cases and 16 of the 18 cases were sensitive to all four drugs. Nine patients who were sensitive to all four drugs were discharged on ATT whereas 7 patients (43.7%) succumbed to the disease. None of the patients with MDR-TBM survived with mortality in such cases being 100%. Discussion Present study evaluated the prevalence of Mycobacterial detection in patients with clinically suspected TBM and further tried to determine the drug sensitivity pattern on all culture positive samples. Thus only 22% of the cases presumptively diagnosed as TBM could be classified as definitive TBM based on case definition. ZN smear and LJ culture conventionally considered as the gold standard for the diagnosis of TBM could detect Mycobacterium tuberculosis from 6% of all suspected cases, thus proved to be a highly insensitive method. BACTEC cultures were positive in 22% of the overall suspected cases. This is distinctly higher yield than the LJ cultures. Few other studies have also reported increased sensitivity of BACTEC cultures in comparison to LJ cultures, especially on extra pulmonary specimens and body fluids[12,13]. Tuberculous meningitis still continues to be a serious childhood illness with a very high incidence of morbidity and mortality. Reported mortality from TBM ranges from 22-27%[5,14]. More than 50% of the patients who survive are left with permanentneurological sequelae[5,14]. The prognosis in cases of multidrug resistance is even worse. Drug resistant TBM usually results from inadequate therapy initially or an inappropriate, incomplete previous anti- tubercular treatment[15]. Presence of co-morbid conditions like diabetes, HIV co- infection, malnutrition, other immuno-suppressive conditions further adds to the complications.Though studies on TBM caused by MDR organisms are limited incidence of multidrug resistant tubercle bacilli is increasing worldwide[7,9-11]. We found almost 18% of the patients (4/22) had MDR-TBM which is similar to another study from India[9]. On further analysis of the associated risk factors it was seen that 2 patients had the presence of risk factors, one patient 25% (1/4) must have taken an inappropriate ATT whereas another patient of MDR–TBM was HIV reactive. Statistical significance could not be ascertained due to the small sample size. Another limitation of the present study was that other associated risk factors and outcome in MDR-TBM cannot be conclusive because of relatively small sample size. Case fatality is higher in cases of MDR-TBM and management has to be individualized. Patients have to be given 2nd line ATT to prevent morbidity and mortality and prevent further transmission of MDR-TBM. Hence all TB meningitis isolates should be cultured and antibiotic sensitivity pattern should be determined. This will help in appropriate management of the patients by optimizing the therapy with second line anti-tubercular drugs. Conclusion Since the prevalence of MDR-TBM as seen in the present study and another study from India is around 18% which is very high. National level surveys involving much larger sample size are needed to define the exact magnitude of MDR-TB. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08050t2.jpg] [pe08050t3.jpg] [pe08050t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}