 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Pediatrics, Vol. 18, No. 4, Dec, 2008, pp. 323-329 Prevalence of Undernutrition of Lodha Children Aged 1-14 Years of Paschim Medinipur District, West Bengal, India Samiran Bisai, MSc, PhD; Kaushik Bose*, MSc, PhD; Anusuya Ghosh, MSc Department of Anthropology, Vidyasagar University, Midnapore, West Bengal, India * Correspondence author; Address: Department of Anthropology,Vidyasagar University, Midnapore- 721102, West Bengal, India E-mail: banda@vsnl.net Received: 10/07/08; Revised: 20/08/08; Accepted: 19/09/08 Code Number: pe08052 Abstract Objective:Childhood undernutrition among tribal children is a serious public health problem in India. The present study was conducted to assess the prevalence of undernutrition (underweight, stunting and wasting) among Lodha children of Paschim Medinipur, West Bengal, India. Key Words:Tribe; Undernutrition; Stunting; Underweight; Wasting; Children Introduction Physical growth in pediatric age is widely used to assess adequate nutrition, health and development of an individual child, and to reflect overall health and nutritional status of a population. It has been well documented that chronic undernutrition is associated with slower cognitive development and serious health impairments later in life that reduce the quality of survival[1]. The majority of deaths in developing countries are associated with undernutrition and occur in children who are only or moderately undernourished[2]. Near about 50% of the children less than five years of age in India are moderately or severely undernourished. These rates are higher in socially and economically underprivileged communities. The tribal populations of India are recognized as socially and economically underprivileged[3]. The vast majority of the tribal populations reside in rural areas of the country. Lodha is one such primitive tribe resident in Paschim Medinipur District of West Bengal, India. According to the latest census, the total population of Lodha is 84966, almost 2% of the total population of West Bengal. More than 95 per cent of Lodhas reside in rural areas. Their mother tongue is Lodha, which is close to Savara, an Austro-Asiatic language. Traditionally, they were forest dwellers, but now they have started cultivation either as owner or as agricultural laborer and are also engaged in hunting and fishing. Thus, they belonged to the low socio-economic class. Therefore, childhood undernutrition is a serious health problem in India including West Bengal. There is a limited data available on health profile and nutritional status among various tribal populations of West Bengal[4-7]. Moreover, there is no information on nutritional status, as assessed by World Health Organization (WHO)[8] recommended Z-score method, among Lodha children. In view of the above, present study reports the prevalence of undernutrition (underweight, stunting and wasting) among Lodha children in Paschim Medinipur district of West Bengal, India. Subjects & Methods This community based cross sectional study was conducted in a village of Paschim Medinipur district – which is situated between Midnapore and Kharagpur towns, about 125km from Kolkata city, the provincial capital of West Bengal. This study was carried out from January to March, 2008. A total of 165 (boys=68, girls=97) children aged 1-14 years were assessed. The children were further divided into two categories:
The estimated number of study subjects for a group was calculated to be 72 by the formula: n=(z2 pq)/d2. Where, z=1.96, p is the prevalence of stunting (25%) among children, q=1-p and d is the desired precision (10%). Therefore, 74 and 91 individuals were selected following simple random sampling method from early and late childhood, respectively. Parents were informed about the objectives of the study and their consent was obtained. The study protocol was approved by the institutional ethical committee. Information on age, gender, weight and height was collected on a pre-tested questionnaire by house to house visit following interview and examination. Anthropometric measurements such as height and weight were made by a trained investigator (AG) following the standard technique[9] using weighing scale and anthropometer rod to the nearest 0.5 kg and 0.1cm, respectively. Children were considered as underweight, stunting and wasting if their weight-for-age, height-for-age and weight-for-height Z-scores below -2.0 SD of the National Center for Health Statistics (NCHS) reference population[10] as calculated using EPI6 software. Severe undernutrition was assessed as Z-score below -3.0 SD. We followed the WHO[8] classification for assessing severity in malnutrition by rate prevalence ranges of these three indicators among children. The classification is shown in table 1. Student’s t-test were undertaken to test for sex differences in height and weight. Proportion test were performed to test for differences in prevalence. Risk ratio (RR) was also calculated. Statistical analyses were performed using the SPSS package and EPI6. Statistical significance was considered as P<0.05. Table 1- Classification assessment for severity of malnutrition by percentage prevalence ranges (WHO 1995)
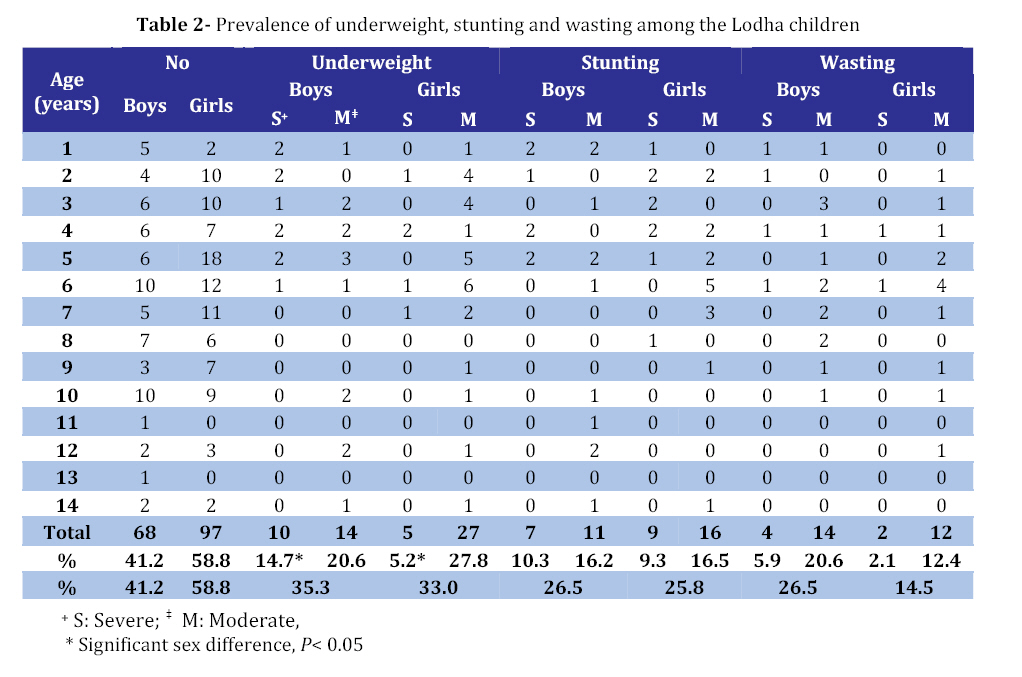
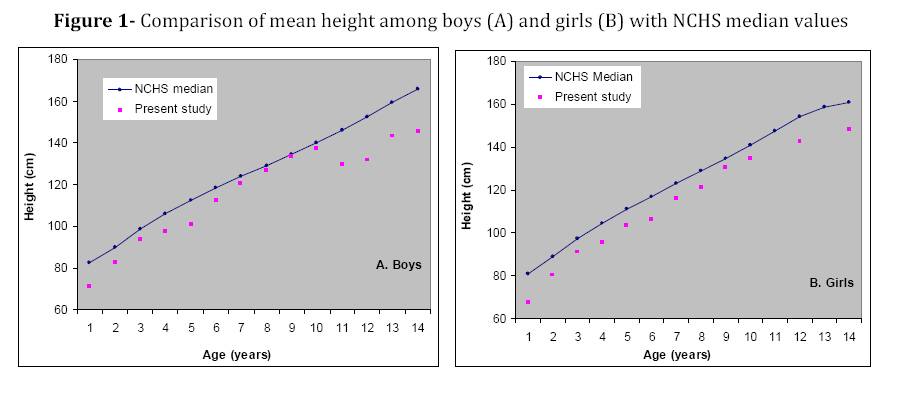
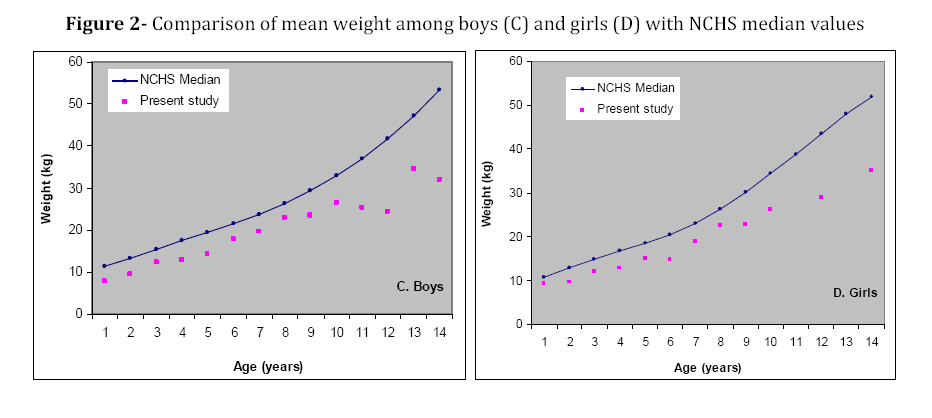
Findings The means weight and height by age and sex were calculated (results not shown in table). It was observed that significant sex difference existed in mean weight and height at age 6 years. Moreover, there was increasing trends in mean weight and height in both sexes with advancement of age. Prevalence of undernutrition (underweight, stunting and wasting) of the studied children is presented in the table 2. Overall (age and sex combined) prevalence of underweight (severe+moderate), stunting and wasting was 33.9%, 26.1% and 19.4%, respectively. Of these, 9.1%, 9.7% and 3.6% children were found to be severely underweight, stunted and wasted, respectively. It is important to note that the rate of severe undernutrition was higher in boys and early childhood (<72 months) compared with girls and late childhood (≥72 months). Similarly, prevalence of underweight, stunting and wasting was higher in boys (35.3%, 26.5%, 26.5%) than their girls (33.0%, 25.8%, 14.5%) counterpart. It is important to note that the prevalence of severe underweight was significantly higher in boys compared with girls (14.7% vs 5.2%, P=0.04). Moreover, the prevalence of underweight (47.3% vs 23.1%) and stunting (35.1% vs 18.7%) was significantly higher in early childhood compared to that during late childhood. They had 2.05 (RR=2.05; 95% confidence interval (CI): 1.31–3.20) and 1.88 (95%, CI: 1.11–3.19) times more chances to be underweight and stunted than during late childhood. Whereas, the prevalence of wasting was similar in both groups (20.3% vs 18.9%; RR=1.09; 95% CI: 0.58-2.02, P> 0.05). Moreover, the rates of severe underweight (early childhood vs late childhood: 16.2% vs 3.3%) and stunting (20.3% vs 1.1%) were significantly higher in early childhood. They had 4.92 (95% CI: 1.44–16.79) fold and 18.45 (95% CI: 2.49-136.42) fold more risk to be an underweight and stunted compared to that during late childhood. According to WHO[8] classification of severity in malnutrition, the overall prevalence of underweight and wasting were very high (≥30% and ≥15%). However, the prevalence of stunting was moderate (20-29 %). Moreover, it is important to note that, among early childhood, the prevalence of stunting (35.1%), underweight (47.3%) and wasting (20.3%) was high to very high, respectively. Discussion Undernutrition is increasingly recognized as a prevalent and important health problem in many developing countries including India. This problem has serious long term consequences for the child and adversely influences development of a nation[11]. Undernutrition continues to be a cause of ill-health and premature mortality among children in developing countries like India[12]. Recent studies have been conducted in different parts of India on health and nutritional status among tribal children and adolescents[13-19]. However, evaluation of nutritional status among the tribal children in West Bengal has not been investigated sufficiently[7]. Our study found that among early childhood, the prevalence of underweight, stunting and wasting were 47.3%, 35.1% and 20.3% respectively. The frequencies of severe underweight, stunting and wasting were 6.2%, 20.3% and 5.4%, respectively. An earlier study[16] from Madhya Pradesh reported very high prevalence of underweight (61.6%), stunting (51.6%) and wasting (32.9%) among Gond pre-school children. The rates of severe underweight, stunting and wasting were 27.2%, 30.1% and 6.5%, respectively. Another study[20] among Kodaku tribal pre-school children of Central India reported frequencies of underweight, stunting and wasting as 59.8%, 43.0% and 35.0%, respectively. The respective frequencies of severe underweight, stunting and wasting were 26.2%, 18.3% and 5.8%. Moreover, the mean height (Fig. 1) and weight (Fig. 2) of the Lodha children of our study were lower than NCHS median values. Thus, these studies clearly indicated that tribals in early childhood were experiencing severe nutritional deficit. This nutritional stress can have implications related impaired cognitive and functional impairment as well as increased morbidity and mortality. In the present study, 33.9%, 26.1% and 19.4% children were found to be underweight, stunted and wasted. An earlier study[7] had reported a similar prevalence (33.7%) of underweight. However, their reported prevalence of wasting (29.4%) was higher than the present study. In contrast, the prevalence of stunting was higher in present study (26.1%) than that reported (17.9%) by Chowdhury et al[7]. In the present study 9.1%, 9.7% and 3.6% children were found to be severely underweight, stunted and wasted, respectively. Chowdhury et al.[7] had reported rates of severe underweight, stunting and wasting as 7.92%, 4.98%, and 9.51%, respectively. These results clearly indicated that the prevalence of stunting was higher among the Lodhas. It has been well documented that stunting is an indicator of chronic or long-term nutritional deficiency[21]. Thus, the children in the present study have been experiencing prolonged nutritional stress. Our study revealed the RR (early childhood versus late childhood) for underweight, stunting and wasting as being 2.05, 1.88 and 1.09, respectively. This implied that early childhood is a greater risk of suffering from undernutrition than during late childhood. Results of pooled data obtained from several studies have shown that children with mild to moderate degrees of undernutrition have a relative risk of 2.2 for death during under five years of age. Furthermore, children with severe undernutrition have a 6.8 fold greater risk for death[22]. One of the limitations of the present study is the small sample size. Further studies are needed among a larger sample of Lodha children for effective planning of nutritional intervention programs in this region. Conclusion Our study demonstrated that the nutritional status of the Lodha children, especially during early childhood of this region is critical. There is an immediate requirement for appropriate steps to be taken to improve nutritional status of this ethnic group. Moreover, it must be mentioned here that similar studies should be undertaken among children of other tribal populations of not only West Bengal but also in other parts of India. Since various tribal groups constitute a sizeable portion of India’s population[23], improvement of their nutritional status is of paramount importance from the national public health perspective. Acknowledgment Financial assistance from Indian Council of Medical Research (ICMR) is gratefully acknowledged. The authors express their thanks to the parents for their help and cooperation.Acknowledgment Financial assistance from Indian Council of Medical Research (ICMR) is gratefully acknowledged. The authors express their thanks to the parents for their help and cooperation. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08052f1.jpg] [pe08052t2.jpg] [pe08052f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}