 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
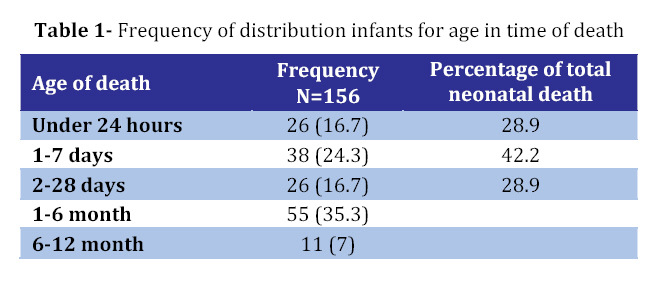
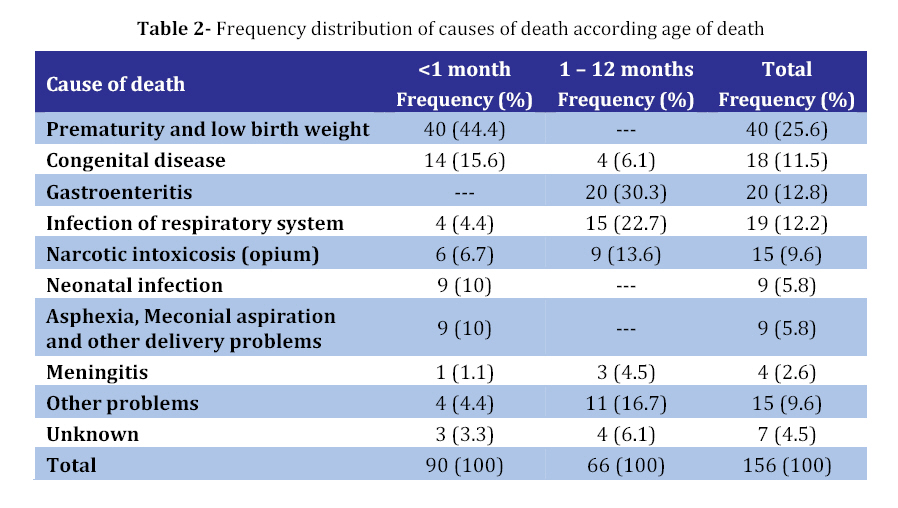
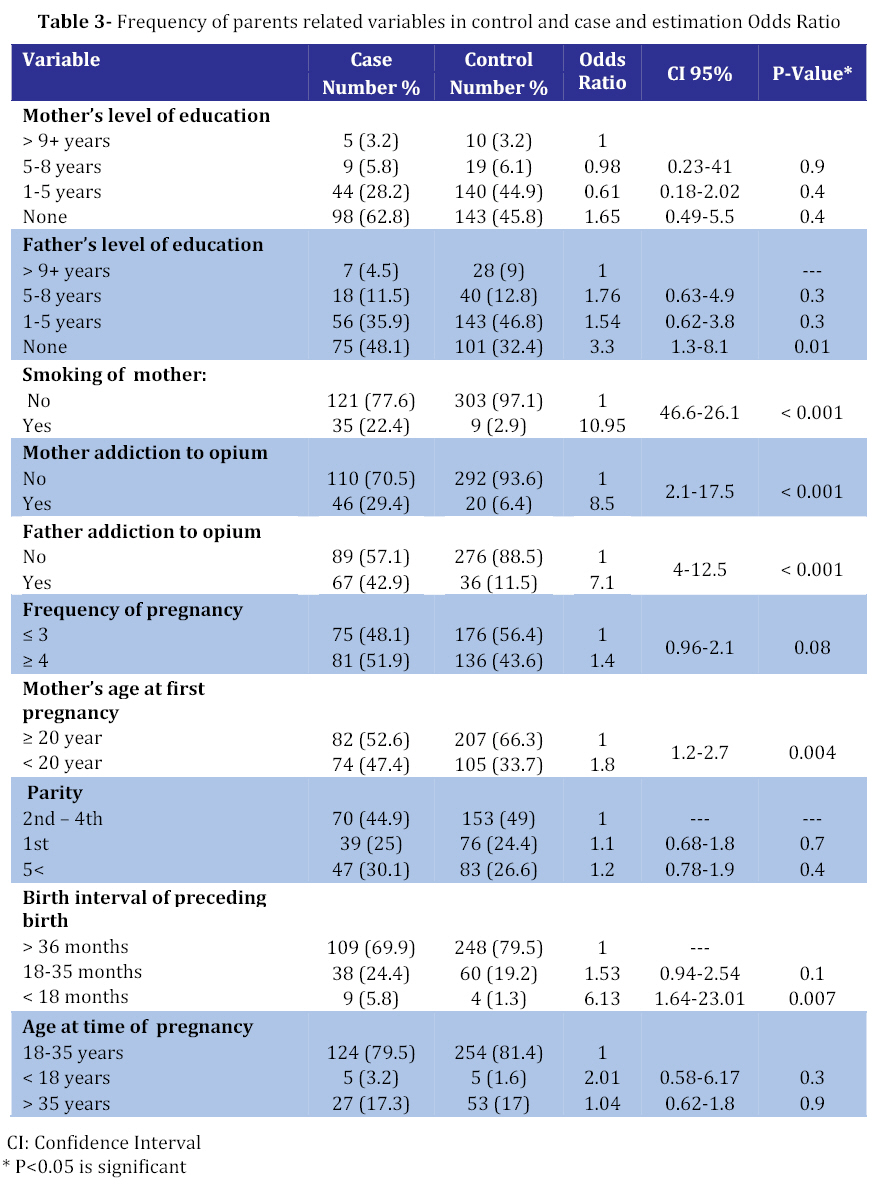
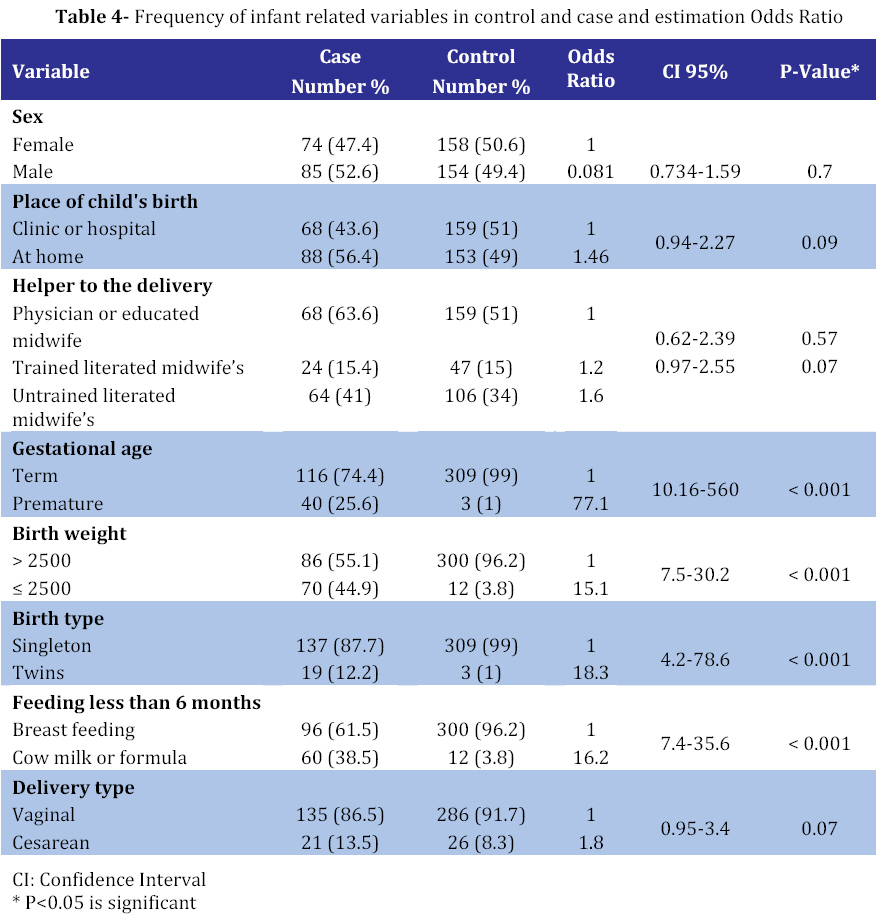
Iranian Journal of Pediatrics, Vol. 18, No. 4, Dec, 2008, pp. 335-342 An Epidemiological Study on Infant Mortality and Factors Affecting it in Rural Areas of Birjand, Iran Gholam Reza Sharifzadeh*1, MSc of Epidemiology; Kokab Namakin2, MD, Pediatrician; Hassan Mehrjoofard3, MSc 1. Department of Social Medicine, Birjand University of Medical Sciences, IR Iran * Correspondence author; Address: Birjand University of Medical Science, Ghafary Ave, Birjand, IR Iran E-mail: rezamood@yahoo.com Received: 17/03/08; Revised: 25/08/08; Accepted: 12/09/08 Code Number: pe08054 Abstract Objective: Infant mortality rate is one of the most expressive indicators of development in all countries. The aim of this study was to determine the cause of infant mortality and risk factors in rural areas of Birjand in Iran. Key Words: Infant; Mortality rate; Health house; Prematurity; Low birth weight Introduction The first year of an infant’s life is of special importance to ensure its health substructure and improve its life quality. Infant mortality rate (IMR) is an important index to demonstrate social health status and mortality rate[1]. IMR is an accepted global indicator of health and socioeconomic status of a given population. While neonatal health is found to be dependent on health care services, post neonatal health is dependent largely on environmental factors. A high IMR, therefore, can indicate unmet health needs and unfavorable environmental factors[2,3]. This statistical index not only indicates the quantity and number of deaths, but is also indicative of life quality. That is why UNICEF maintains that infant mortality rate is certainly one of the most expressive indices of development concept[1], and this significance has taken shape for the fact that the decrease in child mortality is only possible with an improvement in living circumstances of a majority of people. The rise of IMR is attributed to dissatisfied hygienic requirements; and unfavorable environmental factors, economical conditions, environmental sanitation and medical care. Results of similar studies in Iran and other countries have showed that most of infant mortality occurs during neonatal period, especially in the first week[4,5]; and the most important causes of neonatal mortality are prematurity and low birth weight[4-7].On the other hand, during post-neonatal period diarrhea and respiratory infections are the most significant causes[8-11]. Different factors such as social–economic class, mother’s age, birth weight, breast feeding, interval from previous delivery, place of delivery, type of delivery, etc. can influence the possibility of infant mortality[8-10,12-19]. Birjand city (in South Khorasan, Iran) with a rural multitude of 120870 people, with 23 Rural Health centers, and 127 health houses is in charge of offering and primary hygienic-therapeutic services to the rural community. In the year 2001, the rate of infant mortality of 39.7 per 1000 live births, and neonatal mortality rate of 23.3 per 1000 live births have been reported; and regarding the fact that one of the hygienic priorities of Birjand University of Medical Sciences has been a reduction in IMR and Birjand has had the highest ratio of mortality of infants in recent years in Iran and the fact that studying of child mortality plays an important role in health planning in order to reduce the foregoing rate in children[2]. Thus; the main objective of this study was to determine causes of infant mortality and factors associated with it in the rural areas of Birjand. Subjects & methods This Population based case-control study was carried out in a way that cases and controls were selected from a homogenous infant group. Cases comprised of all deaths under 1 year of age recorded between January 2004 and December 2005 inside the health houses sponsored by respective health center. For each case two controls were chosen which had the closest birth time to that of the case and had remained alive up to the age of one year and had already been under the supervision of those health houses. All controls were chosen from family files, on the basis of these criteria. All cases and controls were individually matched with regard to habitation and date of birth. All the death cases, which happened at the age of less than one-year occurred between 2004 and 2005. In health houses, 156 cases were chosen for this study, and two controls per each case (312 live infant controls). Sample size was determined on the basis of sample size formula in case-control studies[20] when P1=0.21 and p0=0.15[5]. The data was collected through questionnaires on the basis of information from family records, interview with mothers and health workers, recording of infants’ cause of death in healthcenters or hospitals. All health houses with infant death cases at the age of less than one year were referred to. In instances at which an infant had died in a health house or hospital under a physician’s supervision, the cause of death was considered on the basis of the physician’s way of supervision. Finally, the cause of death was determined by means of Verbal Autopsy. The present proposal was approved by the research committee of Birjand University of Medical Sciences and relevant ethical aspects have been taken into consideration. The obtained data was fed into SPSS software, and in order to determine effective factors in infants’ mortality and considering the fact that the cases and controls were on the basis of comparing individuals, the data was analyzed by means of Epi-Info 2000 software applying logistic regression analysis method. Findings In this study 156 death cases at the age of less than one year and 312 controls were studied according to the above-mentioned criteria. Out of these death cases, 74 (47.4%) were girls and 82 (52.6%) were boys. As far as the place of death is concerned, 82 (52.6%) cases occurred in a residential village and 4 (2.5%) cases happened in a health center, 61 (39.1%) in the hospital and 9 (5.8%) of them passed away while being transferred to hospital. Table 1 shows frequency distribution of infants’ age in the analysis of infant mortality. As it is observed in the table, 57.7% of the total deaths were neonatal and 42.3% post-neonatal. Out of 90 cases of death under one month (neonatal), 28.9% were during the first 24 hours after birth, 42.2% between 1-7 days, and 28.9% at the age 8-28 days. Table 2 shows frequency distribution of death causes. It is observed that the first cause of death is premature birth and also low birth weight (44.4%), and the second causes are congenital abnormality (15.6%), and opium intoxication (6.7%). The most important causes of post-neonatal mortality were gastroenteritis (30.3%), infection of respiratory system (22.7%) and opium intoxication (13.6%). In order to determine the role of effective factors of infant mortality the effect of every variable on infants’ death was studied separately, by using logistic regression method through Epi-Info 2000 software. The most important of parents related variables and infant related factors are presented in table 3 and 4. Variables of sex, mother’s education level, number of pregnancies, the grade parity, mother’s age at the time of delivery, place of delivery, the person who has helped during delivery, kind of delivery, already mentioned in table 3 and other variables such as mother’s job, father’s job, kinship of parents, number of family members were also taken into consideration; but neither were statistically significant in infant mortality. In this study it was estimated that the risk of mortality of infants whose fathers were illiterate or partially literate was 3.3 times higher than those whose fathers had passed high school or had higher degrees (P= 0.01). Furthermore, factors such as smoking of mother (P<0.001 and OR= 10.95), addiction of mother to opium (P<0.001, OR= 8.5) , age of mother being lower than 20 in the first pregnancy (P=0.004, OR=1.8), interval of two pregnancies less than 18 months (P=0.007, OR=6.13), prematurity (P<0.001, OR=77.1), weight under 25000 gr at birth (P<0.001, OR=15.1), being twins (P<0.001, OR=18.3), and being fed with formula or cow milk (P<0.001, OR=16.2) had significant relation-ship with infant mortality. Discussion In developing countries in under one year age-group mortality is more than 20% of all deaths[3]. About half of these deaths are in the first month after birth (neonatal) and half of these occur in the first week after birth[3]. In this study, out of 156 cases of death of under one year old babies, 57.7% were neonatal and 42.3% post-neonatal. Furthermore, 28.9% of all neonatal deaths occurred in the first 24 hours, 42.2% within 1-7 days, and 28.9% during 8-28 days after birth; these findings correspond with the situation in developing countries. For instance, in the study by Esmail–nasab 54% of neonates’ deaths occurred during the first 24 hours and 21% between the second and seventh day after birth[5]; in a study in Nigeria, 55.1% of deaths under one year occurred at the age of less than one month[4]. So it is recommended to pay special attention to neonatal period and prenatal care. As to the cause of death during neonatal period, the most important factors were prematurity and low birth weight and congenital anomaly. In all scientific texts, too, prematurity and low weight have been presented as the most important factors of infant mortality[4,6,7]. Regarding the cause of post-neonatal death, the most important factors were gastro-enteritis and severe infection of respiratory system; the same as the condition in developing countries. For example, in a study in Egypt 50.5% of the cause of post-neonatal death was diarrhea and 24.8% of deaths were due to respiratory infections[10]. In a study in Saudi Arabia, too, similar results were obtained[11]. The interesting point found in this study was the abundance of death because of opium intoxication that is 6.7% of cases during neonatal and 13.6% during post-neonatal period, while total deaths under one year old was 9.6%. Considering numerous instances of addiction in rural areas of Birjand (in this study it covered 29.5% of cases and 6.4% of controls and it was totally estimated to be 14.1% in the study) and considering the prevalence of the nasty habit of administering opium to infants as soon as they suffer diarrhea or severe respiratory infection, and also addiction of neonates at birth (because of having addicted mothers) it is obviously necessary to pay much more attention to rendering proper health service and medical care, both during pregnancy and after delivery. This study revealed that death risk of addicted mothers’ infants is 8.5 times more than non-addicted mothers'; and as to smoker mothers, it is 10.9 times more than non-smoker mothers'. This not only has bad effects on family economy, but also causes prematurity and low birth weight. These two factors are very important in infant mortality[3]. If the age of mother is under 20 in the first pregnancy (with OR=1.8) it is taken as a risk factor in infant mortality[8,9]; so it is necessary to pay special attention to young pregnant mothers. Another risk factor is short birth interval. In this study it was found that in case birth interval after the previous one is shorter than 18 months, risk possibility would be 6.13 times more than those whose birth interval is more than 36 months and this shows the importance of family population control and taking into consideration the recommended interval (at least 3 years) between two pregnancies. Weight lower than 2500gr at birth, prematurity, being twins and being fed with formula or cow milk have been determined as important risk factors for infant mortality in all scientific texts[12,15-18]. In this study, too, these four variables were determined as strong risk factors for infant mortality. Therefore, it is necessary to provide special medical care for these infants and prevent their deaths by rendering proper training recommendations and medical services. In this study the factors of mother’s education, grade of birth, mother’s age at the time of pregnancy, place of delivery and the kind of delivery didn’t show considerable relationship to infant mortality at the age of less than one year; while in other studies already performed, there has been considerable relationship between these factors and infant mortality[4,5,8,9,10,14,16-19]. The difference is probably due to the different community in this study. One of the limitations of the present study was lack of accurate diagnosis of the cause of death, especially in congenital anomalies, which was not possible due to inadequate facilities in Birjand. Besides, in situations where babies had not died in the hospital Oral Autopsy was utilized to determine cause of death; though it is not a very exact method. Conclusion Considering the fact that many of these variables, which have a significant relationship to infant mortality, are likely to change we can prevent many of these deaths by increasing the level of family information, enforcing family planning, improving pregnancy care, correct referring system, discovering mothers who need special care during and after pregnancy and providing special care for their infants. Acknowledgement We heartily acknowledge education and research deputy of Birjand University of Medical Sciences for the financial support of this project. We are also much obliged to parents cooperating with us in carrying out the study. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08054t3.jpg] [pe08054t4.jpg] [pe08054t2.jpg] [pe08054t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}