 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
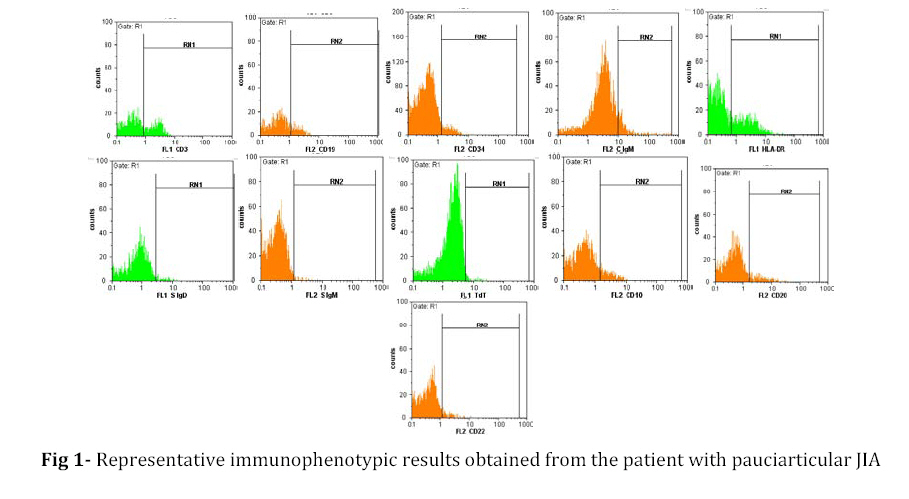
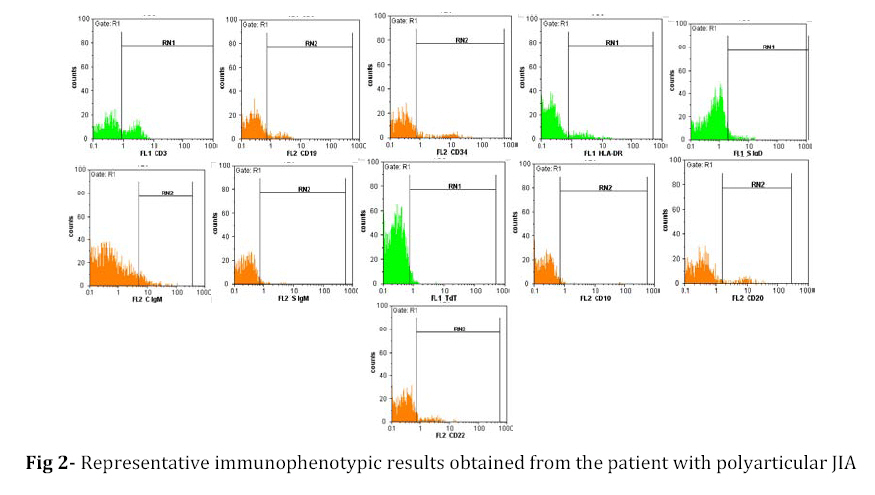
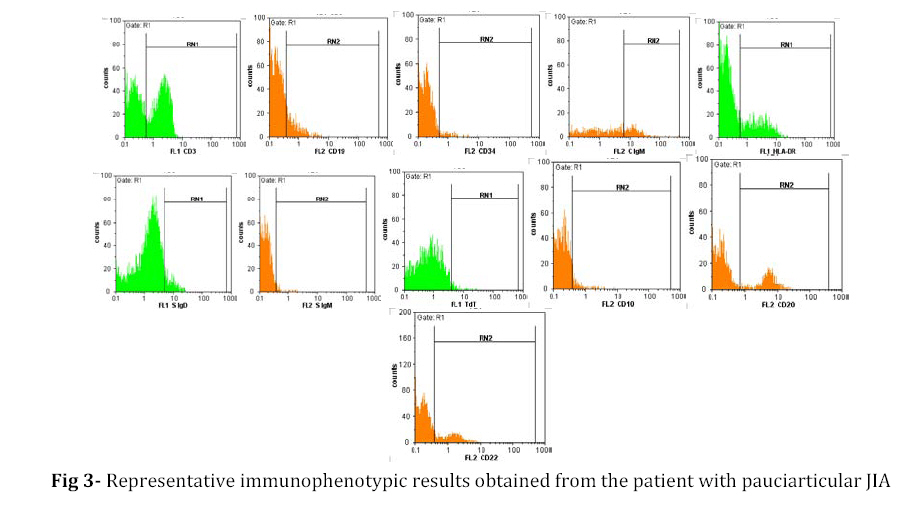
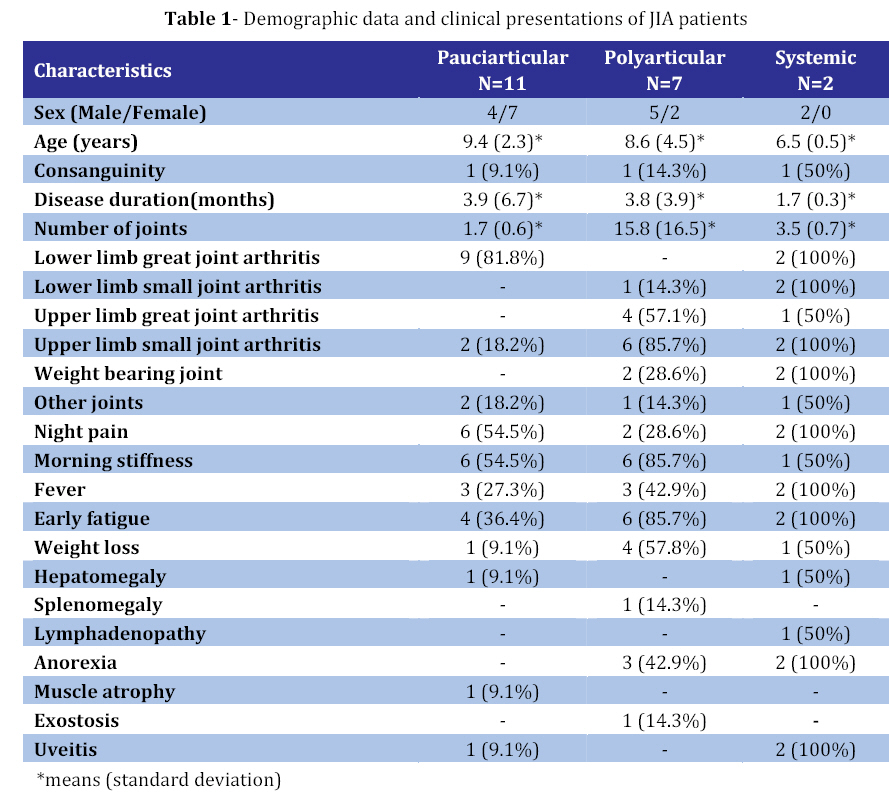
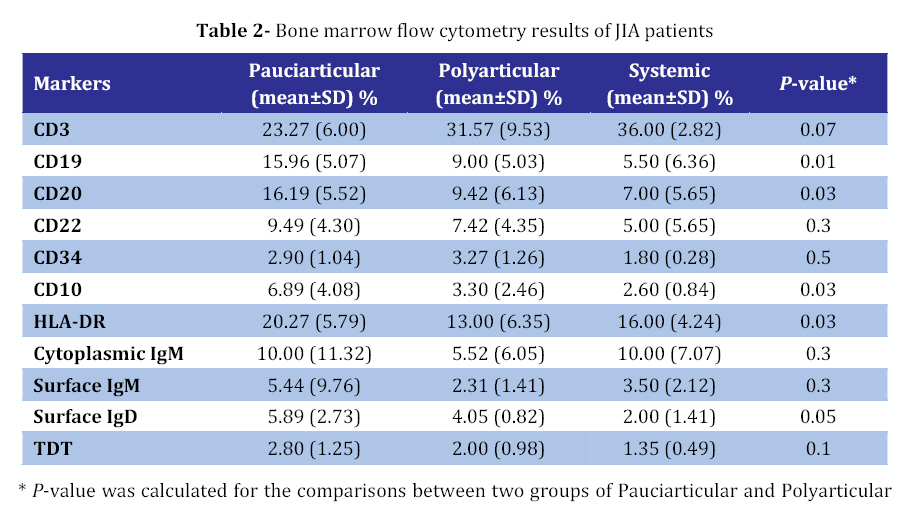
Iranian Journal of Pediatrics, Vol. 18, No. 4, Dec, 2008, pp. 343-350 B-cell Lineage Study in Patients with Juvenile Idiopathic Arthritis Alireza Rezaei1, MD, Pediatrician; Asghar Aghamohammadi*1,2, MD, Pediatric Immunologist; Mohammad Hassan Moradinejad1, MD, Pediatric Rheumatologist; Nima Parvaneh1,2, MD, Pediatrician; Nima Rezaei3, MD; RoheilaSeyedtabaei2, MD; Hossein Asgarian Omran4, MSc; Tahereh Shahrestani4, MSc; Ali Akbar Amirzargar5, PhD 1. Department of Pediatrics, Tehran University of Medical Sciences, IR Iran * Correspondence author; Address: Children’s Medical Center, 62 Qarib St, Keshavarz Blvd, PO. Box: 14185-863, Tehran 14194, IR Iran E-mail: aghamohammadi@sina.tums.ac.ir Received: 02/05/08; Revised: 24/08/08; Accepted: 15/09/08 Code Number: pe08055 Abstract Objective:Juvenile idiopathic arthritis (JIA) is the most common rheumatic disease in children. The exact causes of disease are still poorly understood. It seems that B cells have several functions in JIA, including production of autoantibodies, antigen presentation, production of cytokines, and activation of T cells. Here, we aimed to evaluate B-cell lineage and its precursors in the bone marrow of patients with JIA. Key Words: B-cell Lineage; Immunophenotyping; Juvenile idiopathic arthritis; Chronic Arthritis Introduction Juvenile idiopathic arthritis (JIA) or juvenile rheumatoid arthritis (JRA) is the most common rheumatic disease in children. The term JIA encompasses a group of clinically heterogeneous arthritides that begin before the age of 16, are of unknown cause, and persist for more than 6 weeks[1-3]. Although genetic and environmental components appear to play a role in the pathogenesis of JIA, the exact causes of disease are still poorly understood[2]. While a T cell/macrophage-driven pathology had been considered for JIA, B cell involvement was suggested during 1990s, as B cell-targeted therapies with the use of an anti-CD20 monoclonal antibody (Rituximab) improved the clinical course of JIA[4]. B cells could play either pathogenic or regulatory role in many autoimmune diseases. However, the mechanisms that regulate these B cell functions under different autoimmune settings remain unclear[5]. It seems that B cells have several functions in JIA, including production of autoantibodies, antigen presentation, production of cytokines, and activation of T cells[6,7]. Moreover several alterations in the physiologic process of B cell tolerance have been described in JIA[8-12]. It could be explained through a pathological non-specific "polyclonal" activation which affects both self- and foreign-specific B cells or by self-antigens driving self-reactive B cells, much as foreign antigens stimulate normal B cells[8]. The stage of B cell development at which B cell tolerance is broken in JIA remains unknown. This issue is getting more interesting by considering this fact that some patients with absent mature B cells can develop JIA[9]. Defining the developmental processesthat drive a germinal-cell B cell toward becoming a long-lived bone marrowplasma cell may identify points at which the development of pathogenicautoantibodies can be interrupted. B cells play a variety of immunoregulatory roles through their antigen presentation ability and through cytokine and chemokine production. Innate immune activation of B cells may play a beneficial role in the immunomodulatory functions that provide protection against autoimmunity[10]. So, we decided to evaluate B-cell lineage and its precursors in the bone marrow of patients with JIA in this study. Subjects & Methods Subjects: Twenty consecutive patients with newly diagnosed JIA, who were referred to the Children’ Medical Center Hospital during the year 2007, were enrolled in this study. The term JIA has been widely adopted to describe this heterogeneous group of diseases, following the classification system published by the International League of Associations for Rheumatology[11]. Diagnosis of JIA was based on standard criteria, including: 1) Onset of the disease before the age of 16; 2) Presence of arthritis in one or more joints of the body with associated symptoms such as swelling, restriction and pain during joint movements, and heat on the involved joint; 3) Duration of the disease more than 6 months; 4) Ruling out other causes of juvenile arthritis[3]. JIA is subdivided into three groups of Pauciarticular, Polyarticular, and Systemic JIA according to their characteristics[23]. Systemic JIA is defined by arthritis in one or more joints[12]. Its onset is accompanied by highintermittent fevers and rheumatoid rash as well as other systemicmanifestations. Patients could also have polyarthritis, generally beginning during the firstsix months of disease. ANA and RF are negativein these patients. Polyarticular JIA is defined by arthritis of 5 or more joints, especially small hand joints, in the first 6 months of disease, which is associated with severe joint disability. Pauciarticular JIA is defined with arthritis affecting 1 to 4 joints, especially large joints (knees, ankles, elbows) for the first 6 months of disease[13]. This study was approved by local ethics committee of the hospital. After taking informed consent from the patients, heparinized bone marrow was collected prior to treatment. Immunophenotyping: Bone marrow mononuclear cells were separated using Histopaque (Sigma, USA) density-gradient centrifugation. Isolated cells were washed twice with RPMI 1640 medium (Sigma, USA) prior to immunophenotyping. Using a panel of antibodies against leukocytes antigens, we analyzed the immunophenotype of the JIA patients by flow cytometry to determine the immunologic classification based on the B-phenotype. After separation, the mononuclear cells were stained with a panel of florescent-conjugated mAbs (DAKO, Denmark) specific for B cell lineage [CD10 (clone SS2/36), CD19 (clone HD37) and CD20 (clone B-Ly1)], T cell lineage [CD3 (clone UCHT1)] and non specific lineage [CD34 (clone QBEnd10), HLA-DR (clone AB3) and Terminal deoxy nucleotidyl transferase, TdT (clone HT-6)] (Figs 1, 2, and 3). For surface staining, cells were washed twice with phosphate buffer saline (PBS) and after incubation of 106 cells with 10 μl of mAb at 4ºC for 30 minutes, cells were washed twice with phosphate buffered saline (PBS 0.15M, pH 7.2) before scanning by flow cytometer (Partec, Germany). In addition, staining for TdT and IgM were performed at the cytoplasmic level. The same method was used for intracytoplasmic staining, but before addition of mAb, cells were made permeable using permeabilizing solution (DAKO, Denmark) and then were washed with PBS. Forward and side-scatter gates were used for analysis of leukemic antigenic expression. Sample analysis and data acquisition were performed by Flomax flow cytometry analysis software (Partec, Germany). The criterion for surface marker was expressed positively by at least 20% of the leukemic blast cell population after subtraction of background staining with isotype-matched conjugated mAbs of irrelevant specificity. Statistical Analysis: Data analysis was performed using SPSS statistical software package (version 14.0). Statistical differences of various clinical and laboratory parameters between groups were evaluated by Chi-square or the Fisher’s exact tests. Independent-samples t test was performed to compare the means between the groups. P-values less than 0.05 were considered significant. Findings Characteristics of the Patients: Twenty patients (11 male and 9 female), with the age range of 3 to 15 years (median 9 years), who were referred to the Children's Medical Center Hospital during 2007, were enrolled in this study. Pauciarticular JIA was the most common type, which was seen in 11 cases (55%). Polyaticular JIA was seen in 7 cases (35%), whereas Systemic JIA was only detected in two cases. The duration of the disease was between 1.5 to 24 months (median 2 months). Clinical Presentation: Lower limb great joint arthritis was the most common involvement in the JIA patients, which was seen in 18 cases (90%), followed by morning stiffness (13 cases), early fatigue (12 cases), night pain (10 cases), fever (8 cases), upper limb small joint arthritis (8 cases), weight loss (6 cases), anorexia (5 cases), upper limb great joint arthritis (5 cases), and arthritis of the other joints (4 cases). Hepatomegaly, weight bearing joint arthritis were also seen in 2 cases, whereas lower limb small joint arthritis, muscle atrophy, uveitis, lymphadenopathy, splenomegaly, exostosis were each seen in only one case. Table 1 presents clinical findings of the patients in each group of disease. Although great joints were commonly involved in the patients with pauciarticular JIA, the difference was not significant; however, small joints were significantly involved more common in the polyarticular JIA in comparison with pauciarticular JIA (100 vs. 18.2%, P=0.002). Immunophenotype: Flow cytometric study of bone marrow showed in comparison with normal range[12-14]that 15 cases had low levels of CD10, 14 cases had low levels of CD19, 6 cases had low levels of CD20, and 2 cases had low levels of HLA-DR. Both cases of systemic JIA had low limits of CD10, CD20, CD19, CytIgM, SIgM, SIgD, and normal levels of CD34, CD3 and HLA-DR. Six of 7 patients with polyarticular JIA had low levels of CD10, CD19, SIgD, and CytIgM. Although 10 of 11 patients with pauciarticular JIA had also low levels of CD10, there was significant difference between mean CD10 percentage of the two groups (6.89±4.08 in pauciarticular vs. 3.30±2.46 in polyarticular, P=0.03). The mean CD19 and CD20 percentages in polyarticular JIA patients were significantly lower than the pauciarticular JIA patients (9.00±5.03 vs.15.96±5.07 for CD19, P=0.01; 9.42±6.13 vs. 16.19±5.52 for CD20, P=0.03). The mean HLA- DR percentage in polyarticular JIA patients was also significantly lower than in the pauciarticular JIA patients (13.00±6.35 vs.20.27±5.79, P=0.03) (Table 2). Discussion JIA is a complex disease characterized by progressive destruction of the joints and the synovial hyperplasia, activation of the immune system and chronic inflammation. JIA is a disease of unknown etiology with a significant burden in terms of morbidity and disability[11]. There are several evidences indicating B-cell involvement in JIA pathogenesis. Decreased B cells and increased autoantibodies in the peripheral blood in association with hypergamma-globulinemia due to B cell hyperactivity in JIA patients[15], the effective role of Rituximab, a chimeric anti-CD20 monoclonal antibody, in B cell depletion therapy in RA and other autoimmune diseases[16], occurrence of JIA in patients with common variable immunodeficiency who have defects in antibody formation[17] and also in patients with X linked agammaglobulin-emia who are absent for mature B cells[9], are all theories that note the role of B cell differentiation defects in JIA patients. In our study by comparing the results taken from bone marrow flow cytometry, with the normal range of B cell lineage markers[12-14], had shown low levels of CD10, CD19, CD20, CytIgM, SIgM, SIgD in both cases of systemic JIA patients. Although These findings have not been reported previously in patients with JRA in the literature, peripheral blood flowcytometric analysis in A 5-year-old girl with systemic onset of JRA had shown that CD19+ and CD20+ B lymphocytes ratios were absent[18]. Some cytokines secreted from T cells may stop the maturation and differentiations of CD19+ and CD20+ B lymphocytes. Autoantibodies against the antigenic B cell determinants may be the cause of absence of B cells[19]. In above 80% of polyarticular and pauciarticular patients in our study low levels of CD10, CD19, CytIgM, SIgD were detected. The importance of these findings is unknown for the etiology but could suggest defect in the pre, pro, immature and mature B-cell differentiation. Another study, suggests that there may be a population of circulating B cells in patients with JRA and other rheumatic diseases which is sufficiently mature to differentiate and secrete immunoglobulin in response to cytokines alone[20]. In our study, the patients with pauciarticular JIA predominantly had lower limb great joint involvement, whereas the polyarticular JIA patients predominantly had upper limb small joint involvement. Considering such differences between phenotypes of different groups of JIA, various underlying pathophysiologies could be suspected. In our study, significant differences in CD10 of bone marrow were detected between the polyarticular and pauciarticular groups. CD10 are pre B ell markers. So, as of lower level of this marker in polyarticular JIA, it seems that polyarticular JIA patients had lower percentage of pre B ell stage. These significant differences in CD19, CD20, and HLA-DR of bone marrow also were detected between the groups. Although such findings were not previously reported, difference in HLA-DR presentations between these two groups was described before[21]. In fact polyarticular JIA patients had lower level of CD19, CD20 than pauciarticular JIA patients that could suggest decrease of B cell precursor in bone marrow is one of mechanisms for pathogenesis of JIA. JIA patients had low levels of CD10, CD19, CD20. polyarticular patients had lower levels of D10, CD19, CD20 than pauciarticular JIA patients and systemic onset JIA patients had lower levels than both of them. Conclusion In conclusion, decreasing of B cell precursor in bone marrow is one of mechanisms for pathogenesis of JIA and the more B cell precursor in bone marrow decreased, the worst is the severity of the disease. However, the findings of this study should be substantiated in future studies with more patients and using more B cell lineage specific markers. Acknowledgment This study is performed with a grant made to Mohammad Hassan Moradinejad by Tehran University of Medical Sciences. The authors thank the patients and their families for their contribution to the study. References
© Copyright 2008 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe08055t1.jpg] [pe08055t2.jpg] [pe08055f2.jpg] [pe08055f1.jpg] [pe08055f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}