
|
Iranian Journal of Pediatrics
Tehran University of Medical Sciences Press
ISSN: 1018-4406 EISSN: 2008-2150
Vol. 18, Num. 4, 2008, pp. 351-356
|
Iranian Journal of Pediatrics, Vol. 18, No. 4, Dec, 2008, pp. 351-356
Post BCG Lymphadenitis in Vaccinated Infants in Yazd, Iran
Mostafa Behjati* 1, MD, Pediatrician; Jamshid Ayatollahi 2, MD, Infectious specialist
1. Department of Pediatrics, Shahid Sadoughi University of Medical Sciences, Yazd, IR Iran
2. Infectious Diseases Department, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
* Correspondence author;
Address: Afshar Hospital, Jomhoori Islami Blvd, Yazd, IR Iran
E-mail: dr_behjati@yahoo.com
Received: 17/01/08; Revised: 21/05/08; Accepted: 25/07/08
Code Number: pe08056
Abstract
Objective:Bacille Calmette-Guَerin (BCG) vacination is performed as a part of expanded program of immunization (EPI). Lymphadenitis is the most common complication of BCG vaccination. The aim of this study was to determine the incidence and natural course of BCG lymphadenitis vaccinated in Yazd, Iran.
Methods:In this analytical prospective follow up study a total of 480 (240 females and 240 males) consecutive newborns received 0.05 ml of BCG vaccine intradermally on right arm within the first week of life during April to July 2003. These babies were followed up when 1.5, 3, 4.5, 6 and 9 months old.
Findings:A total of 26 (5.8%) cases of lymphadenitis were detected. Lymphadenitis occurred as ipsilateral axillary nodes in 24 (92.3%) cases, supraclavicular in one (3.8%) case, and supraclavicular in association with axillary nodes in one case (3.8%). Infants developed lymphadenitis during 4 wks of life in one (3.84%) case, between first and fourth month of life in 14 (53.8%) cases, and between fourth and sixth month of life in 11 (42.3%) cases. All 26 cases of lymphadenitis were followed up for 9 months. Twenty two (84.6%) cases were simple or non-suppurative and 4 (15.4%) cases suppurative lymphadenitis. Eleven (42.3%) cases of non-suppurative lymphadennitis showed spontanous resolution and eleven (42.3%) cases had partial regression without progression or drainage. Four (15.4%) cases developed suppuration with one (3.8%) case of fistulation and drainage.
Conclusion:The greater incidence of lymphadenopathy in our cases can probably be attributed to a more immunogenic vaccine (Pasteur institute, Tehran), young vaccinees (newborn infants), injection in the right arm or improper dilution. Non-suppurative BCG lymphadenitis is a benign condition and regresses spontanously without any treatment.
Key Words: BCG; Lymphadenitis; Vaccination;Immunization; Tuberculosis;Infants
Introduction
Tuberculosis (TB) remains a major, global public health problem, particularly in low-income countries. The most serious complication of tuberculosis in children is meningoencephalitis, which is associated with high mortality and morbidity rates[1]. The Bacille-Calmette-Guerin (BCG), a living attenuated vaccine with characteristic residual virulence, has been used to prevent tuberculosis since 1921.The world health organization (WHO) has recommended BCG Vaccination as apart of the global expanded program for immunization (EPI) in developing countries[2]. Though, the efficacy of BCG-Vaccine against tuberculosis is uncertain, it is generally agreed that the vaccine is protective against the meningeal/miliary TB in childhood tuberculosis[3].
BCG is a live attenuated vaccine and is being given routinely to all newborns under the universal immunization program. BCG vaccine induces delayed type of hypersensitivity (DTH) reaction and cell-mediated immunity in the host 4-8 weeks after vaccination [4].
After interadermal injection, BCG start multiplying rapidly at the site of inoculation and later is transported through the lymphatics to the regional lymph glands, followed by heamatogenous dissemination resulting in creation of very small foci in different organs. This is also called normal BCGitis in the course of successful BCG vaccination[5].
Although BCG vaccination often results in local adverse reactions, serious complications are rare, therefore BCG vaccine is considered as safe method of tuberculosis prevention. Lymphadenitis is the most common complication of BCG vaccination[5, 6].
There are two forms of BCG lymphadenitis in natural course of lymphadenopathy. Simple or non-suppurative lymphadenitis which usually resolves spontaneously within a few weeks, and suppurative lymphadenitis, which characterized by appearance of fluctuation with erythema and edema of the overlying skin[5].The aim of this study was to determine the incidence and natural course of BCG lymphadenitis in infants vaccinated in Yazd/Iran.
Subjects & Methods
This is an analytical prospective follow up study. The researcher visited all seven maternal and child health centers where BCG and other vaccinations are carried out, and received the data from nurses trained for BCG vaccination and the responsible pediatrician.
Totally 480 (240 boys and 240 girls) consecutively born neonates with normal birth weight (>2500g birth weight) and low birth weight (<2500g birth weight) (excluding premature newborns) received during April to July 2003, 0.05ml (0.05mg) BCG vaccine (manufactured by Pasteur institute, Tehran). BCG vaccine was given as a single intradermal injection over the deltoid muscle of the right arm.
At the same time trivalent oral polio and hepatitis B vaccines were administered according the national immunization program. These babies were followed up in immunization clinic when 1.5, 3, 4.5, 6 and 9 months old to observe lymphadenitis in axillary, supraclaricular and cervical area at the ipsilateral and contralateral BCG vaccination sides. Thirty one infants did not appear to follow up, 449 infants (229 females and 220 males) were available for final analysis. A lymph node sized 10 mm or more was regarded as lymphadenitis or lymphadenopathy.
BCG lymphadenitis was diagnosed by pediatrician. Criteria for diagnosis of BCG lymphadenitis were:
- Isolated axillary (or rarely supraclavicular/ cervical) lymph node enlargement
- history of BCG vaccination on the same side
- absence of tenderness and raised temperature over the swelling
- absence of fever and other systemic symptoms
Chest radiography, mantoux reaction, and hematological analysis are not helpful. Fine needle aspiration cytology corroborates the clinical diagnosis in doubtful cases.
SSPS software was used for data entry and analysis. Data were tested for statistical significance using the chi-squared, ANOVA, and fisher exact test, with P-value considered statistically significant at the 0.05 level. This study was approved by the local ethics committee of medical research council.
Findings
Four hundred eighty (480) babies, were born at the hospitals in Yazd, Iran during April to July 2003. Thirty one infants were excluded from study because questionnaire was not complete. Four hundred forty nine (449) infants (229 females and 220 males) were available for final analysis.
Totally 26 (5.8%) cases of lymphadenitis were detected consisting of 14 (6.4%) male and 12 (5.2%) female infants. There was no statistically significant difference (P=0.61) between male and female infants. Of the 449 newborns, 33 (7.3%) were low birth weight (≤2500g). Two cases (6.1%) of lymphadenitis occurred in this group. There was no statistically significant difference (P=1, 95% CI 4.25-4.29) between rates of post BCG vaccine lymphadenitis in low birth weight (6.1%) and normal weight infants (5.8%). Also relative risk ratio of BCG vaccine lymphadenitis was calculated between low birth weight and normal birth weight. There was no statistically singnificant relationship between BCG vaccine hymphadenitis (RR=1.051, 95% CI 0.26-4.25) and low birth weight or normal birth weight. The regional distribution of lymphadenitis showed in 24 (92.3%) cases ipsilateral axillary nodes, in one (3.84%) case right supraclavicular and in one (3.84%) case, right supraclavicular in association with right axillary nodes.
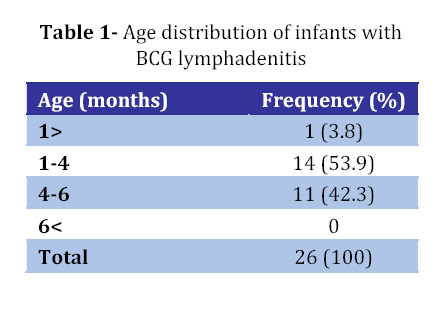
The lymphadenitis appeared in one (3.84%) case during 4 weeks of life, but in most cases within six months (Table 1). The first follow-up physical examination of the 26 children with lymphadenitis took place at the age of 1.5 months. Subsequent examinations followed at 3, 4.5, 6 and 9 months of age to observe the natural course of lymphadenitis. Lymph nodes sized 1-4 cm.
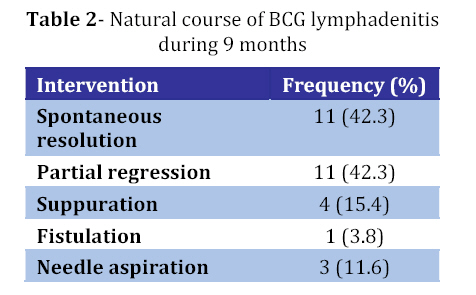
Eleven (42.3%) cases had spontaneous resolution and 11 (42.3%) cases had partial regression without progression and drainage. Four (15.4%) cases developed suppuration, of which 3.84% developed fistulation and drainage. Three (11.56%) cases of suppurative lymphadenitis underwent needle aspiration (Table 2). There was no statistically significant difference between male and female cases (P=0.61, 95% CI 4.69-6.89).
Discussion
The only available vaccine against tuberculosis is the Bacille Calmette Guerin, named after two French investigators responsible for its development[4,7]. The original vaccine organism was a strain of Mycobacterium bovis attenuated by subculture every 3 weeks for 13 years[8]. Canadian Immunization Guide has recommended BCG vaccination in countries where the incidence of tuberculosis infection is more than 1%[9]. BCG vaccination is recommended routinely for all newborns in the universal immunization program in these countries[4]. BCG vaccine has low incidence of serious adverse reactions, and is considered to be a safe vaccine[5,10,11].
Lymphadenitis is the most common complication of BCG vaccination[5,10,12]. Lymphadenitis accounted for about 98% ofcomplications; the remaining 2% consist of abscess, ulceration, and arthritis[13]. BCG related lymphadenitis is characterized by regional lymph nodes enlargement, ipsilateral to the site of administration, with no other identifiable cause for lymphadenopathy. Absence of fever, tenderness, and other systemic symptoms differentiates it from pyogenic adenitis. Differentiation from tuberculous lymphadenitis may be difficult, but cases of isolated axillary glandular tuberculosis are very rare.
Our study includes 449 infants who received 0.05 ml of BCG vaccine. The prevalence of lymphadenitis in our study was 5.8%. This proportion is higher than reported from Canada 1%[14], Chile 0.7%[15], Turkey 0.7%[16], Jamaica 1.9%[17], South Africa 0.5%[18], and in some other studies[7,8,13], but lower than in India[19]. In a study in Semnan/Iran prevalence of lymphadenopathy, suppurative lymphadenitis and fistulization was 2.2%, 0.5% and 0.18% respectively[20]. This was lower than observed in our study. In another study in Hamadan/Iran, prevalence of regional lymphadenitis following BCG vaccination in neonates was 5.0%[21]. This is almost consistent with that of the present study (5.8%).
There is no agreed definition as what constitutes to BCG lymphadenitis, particularly with regards to the size of lymph node enlargement and its time of onset after vaccination[22]. In our study, lymph nodes sized 1 cm or over, were regarded as lymphadenitis.
In present study, there was no statistically significant difference between male and female gender, but in a few reports the prevalence of lymphadenitis is higher in male than in female gender[19,23].
In present study 84.6% patients had spontaneous regression and resolution of lymphadenitis without progression and drainage. Suppurative lymphadenitis is much less common than lymphadenopathy occurring in 15.4% cases of all infants with lymphadenitis and 0.87% of BCG vaccine recipients. This being higher than that reported Hamadan Iran[21], Semnan-Iran 0.54%[20], Riodojaniro-Brazil 0.3%[24], south Africa 0.18[18], Turkey 0.3%[16]. In our study incidence of suppurative lymphadenitis was 15.4% of all infants with lymphadenitis. This result was consistent with another study in India (Suppuration 15%)[19]. The incidence of suppurative lymphadenitis was significantly higher in vaccinated infants with lymphadenitis in Korea[12] 41.2% and in Zimbabwe 62%[25]. Once suppurative has supervened, the subsequent course is usually distinguished by the occurrence of spontaneous discharge and sinus formation. Non suppurative BCG lymphadenitis follows a benign course in most individuals. Most of the cases regress spontaneously with conservative management.
In our study lymphadenitis developed within 6 month in 26 cases (100%) and none of children developed lymphadenitis 6 month after the vaccination. In a study this result was 92% of cases[26]. In our study the most of cases was appeared within 4-16wk, whearease in other studis[20,26], the most of cases was appeared within 8 wk and a few case developed 1 to 5 year after the vaccination[26]. An incidence of 0.1 per 1,000 vaccinated children was observed in Denmark and developing countries up to five of 1,000 children are affected[27]. Adverse reactions are more common in young infants[9]. In one study the localization of lymphadenopathy varied according to vaccination sit; left axilla (n=57), left supraclavicular region (n=2) and right inguinal region (n=1)[26], whereas in our study the most of region was right axillary area, because in Iran site of vaccine injection is right arm just above the insertion of the deltoid muscle.
In our study, the regional distributions of infant with lymphadenitis were in concordance with study of Singla A, et al and Coraya JS, et al[ 5, 19]. The majority of studies reported which rate of BCG lymphadenitis following interadermal injection in left arm less than injection in right arm[21, 28, 29].In our study higher incidence of lymphadenitis can be due to site of injection (right arm versus left arm). Risk of lymphadenitis is higher if vaccine is given during the newborn period[5]. In present study higher incidence of lymphadenitis can be due to young age of recipient (newborn period). BCG is not easy to adminidter as an intradermal injection at any age, but especially to a newborn. The commonest mistake is to give the injection too deep, failing to raise the classical orange-skin appearance in dermis. In present study higher incidence of lymphadenitis may be due to improper technique in administration.
The occurrence of adverse events associated with the vaccine is related to concentration of bacilli in the vaccine, child’s age, strain and vaccination method[26,27,30]. The younger children are more commonly affected[25].In present study the higher incidence of lymphadenitis, can be due to strain of BCG (Iran strain versus, Japan, Moscow strains), age of recipient (Newborn infant versus older children), site of injection (Right arm versus left arm) and are frequently related to improper technique in administration (mainly improper dilution) and secondary to probably introduction of more immunogenic vaccines.
Conclusion
In our study, the greater incidence of lymphadenitis can be due to vaccine strain (Pasteur institute, Tehran), young vaccinees (newborn infants), improper technique in administration (mainly improper dilution), right arm injection and secondary to introduction of more immunogenic vaccines. It is important to develop uniform system to standardize BCG vaccines and exercise restrain in switching the preparations of BCG vaccine in the developing countries, as this could influence the compliance to EPI programs in these countries. The most common form of BCG lymphadenitis is simple or non-suppurative. Non-suppurative BCG lymphadenitise is a benign condition and regresses spontanously without any treatment.
Acknowledgment
This study was supported by Medical Research Council and Infectious and Tropical Disease Research Center, Shahid Saddughi University of Medical sciences. We thank Hossein Ahmadieh for statistical analysis.
References
- Styblo K, Meiger J. Impact of BCG Vaccination program in children and young adults on the tuberculosis problem. Tuber Lung Dis J. 1976;57(1):17-43.
- Lugosi L. Theoretical and methodological aspects of BCG Vaccine from the discovery of Calmette and Guerin to molecular biology.A review.Tuber Lung Dis J. 1992; 73(5):252-61.
- Bonmon MJ. BCG and Tuberculosis, Arch Dis Child. 1999;80(1):80-3.
- Kaur S, Faridi M M A, Agarwal KN, BCG Vaccination reaction in low birth weight infants, Indian J Med Res. New Delhi. 2002;116:64-69.
- Goraya JS, Virdi VS, Bacilli calmette- Guerin lymphadenitis. Postgraduate Med J London. 2002;78(920):327-9.
- Milstien JB, Gibson JJ. Quality control of BCG Vaccine by WHO: a review of factors that may influence Vaccine effectiveness and safety. Bull WHO. 1990;68(1):93-108.
- Barouni AS, Augusto C, Queiroz MVNP, et al. BCG Lymphanopathy detected in a BCG vaccinated infant. Braz J Med Biol Res. 2004;37(5):697-700.
- Starke JR, Munoz F. Tuberculosis, BCG Vaccination. In: Kliegma RM, B ehrman RE, Jenson HB, (eds).Nelson Textbook of Pediatric. 17 ed. Philadelphia; Saunders. 2004; Pp:958-72.
- Langley J, Ellis E, Deeks S, National Advisory Committee on Immunization; Health Canada First Nations; Inuit Health Branch. Statement on Bacille Calmette Guérin (BCG) vaccine. Can Commun Dis Rep. 2004;30:ACS-5.
- Gołebiowska M, Andrzejewska E, Stryjewska I, et al. Adverse events following BCG vaccination in infants and children up to 36 months of age.Przegl Epidemiol. 2008;62(1):71-5.
- Szczuka I. Adverse event after BCG Vaccination in Poland in the years 1994-1997. Pneumonol Alergol Pol. 1999;67(5-6):208-16.
- Baek HC, Chang JY, Moon SJ, Oh SH. Lymphadenitis following interadermal BCG vaccination. Korean J Pediatr. 2006; 49(1):46-50
- Award R. BCG Vaccine and post BCG Complications among infant in Gaza strip1999.East Mediter Health J. 2001; 7(1-2): 221-220.
- Evaluation of BCG vaccination programmes. Weekly Epidemiological Records. 1982;57(16):121-123
- Tidjani O, Amedome A. The protective effect of BCG vaccination of the newborn against children tuberculosis in an African community. Tubercle. 1986;67(4):269-81.
- Sirinavin S, Chotpitayasunondh T, Suwanjutha S, et al. Protective efficacy of neonatal Bacillus Calmette-Guerin vaccination against tuberclosis. Pediatr Infect Dis J. 1995;10(5):359-65.
- Praveen KV, Smikle MF, Prabhakar P. Outbreak of BCG vaccine associated lymphadenitis and abscess in Jamaica. Pediatr Infect Dis J. 1990;9(12):890-3.
- Jeena PM, Chhagam MK, Topley J, et al. Safety of the intradernal BCG vaccine in neonate in Durban, South Africa. Bull WHO. 2001;79(4):337-43.
- Singla A, Singh S, Goraya JS, etal. The natural course of BCG lymphadenitis. Pediatr Infect Dis J. 2002;21(5):446-8.
- Seyfhashemi M, Hemati A, Mazaheri M, et al. Complications of BCG vaccination in children. Iran J Pediatr. 2005;15(3):210-4. (Article in Farsi)
- Saba MS, Farshchian M, BCG adenitis Hakim Res J. 1999;2(2):84-7. (Article in Farsi)
- Stone MM, Vannier AM, Storch, SK, etal. Brief report, Meningitis due to iatrogenic BCG infection on two imunocompromised children. N Eng J Med. 1995;333(9):561-3.
- Mori T, Yamauchi Y, Shiozawa K. Lymph node swelling due to BCG Vaccination with Multipuncture method. Tuber Lung Dis. 1996;77(3):769-73.
- Lanchriet C, Levy-Bruhl D, Bingono E. Efficacy of BCG vaccination of the newborn: evaluation by a follow-up study of contacts in Bangui. Int J Epidemiol. 1995;24(5):1042-9.
- Ray CS, Pringle D, Legg W, et al. Lymphadenitis associated with BCG vaccine: A report of an outbreak in Harare Zimbabwe. Cent Afr J Med. 1988;34(12): 281-6.
- Nazir Z, Qozi SH. Bacillus Calmett- Guerin (BGC) lymphadenitis– Changing Trends and management. J Ayub Med Coll Abbottabab. 2005;17(4):16-8.
- Bareto Ml, Pereira SM, Fereiera AM, BCG vaccine: efficacy and indication for vaccination and revaccination. J pediatr (RioJ). 2006; 82 (3 supple):S45-54.
- Masjedi MR. Guideline for the fight against tuberculosis, Tuberculosis Research Center of Iran, Tehran, Shahid Beheshti Univercity of Medical Sciences, 1996; P: 43 (Book in Farsi).
- WHO Tuberculosis research office suppurative lymphadenitis following intradermal BCG vaccination of preschool children. Bull WHO. 1995;12(1-2):143-67.
- Bolger T, O’Connell M, Menon A, et al. Complications associated with the bacille Calmette Guérin vaccination in Ireland. Arch Dis Child. 2006;91(7):594-7.
© Copyright 2008 - TUMS PUBLICATIONS
The following images related to this document are available:
Photo images
[pe08056t1.jpg]
[pe08056t2.jpg]
|

{kind=link}
{kind=link}