
|
Iranian Journal of Pediatrics
Tehran University of Medical Sciences Press
ISSN: 1018-4406 EISSN: 2008-2150
Vol. 18, Num. 4, 2008, pp. 373-376
|
Iranian Journal of Pediatrics, Vol. 18, No. 4, Dec, 2008, pp. 373-376
Colocolic Intussusception without Lead Point; A Case Report and Literature Review
Rahim Mahmudloo1, MD, Thorax Surgeon; Shahsanam Gheibi*2, MD, Pediatric Gastroenterologist; Sona Nuri Vahed3, MD, Internists
1. Department of Surgery, Urmia University of Medical Sciences, IR Iran
2. Department of Pediatrics, Urmia University of Medical Sciences, IR Iran
3. Department of Internal Medicine, Urmia University of Medical Sciences, IR Iran
* Correspondence author;
Address: Department of Pediatrics, Shaheed motahhari Hospital, Urmia, IR Iran
E-mail: drgheibi@umsu.ac.ir
Received: 17/01/08; Revised: 04/05/08; Accepted: 04/06/08
Code Number: pe08060
Abstract
Background:Colocolic intussusception is rare in children and most cases in adolescents are produced by a lead-point. A review of the English-written literature revealed only three cases of colocolic intussusception without lead point.
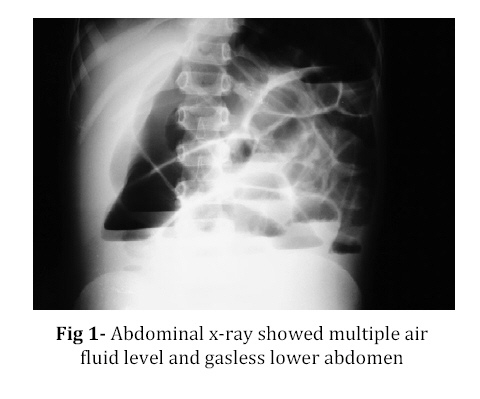
Case presentation:A seven year-old boy with chief complaint of colicky abdominal pain and vomiting for five days, dysentery for 4 days, and no response to antibiotic therapy, increasing pain and abdominal distension was referred to pediatric gastroenterologist. Abdominal x-ray revealed multiple air-fluid levels and gasless colon. Pseudo-kidney appearance was reported in abdominal ultrasound at splenic flexure. Colocolic intussusception diagnosis without any lead point was confirmed in laparotomy and reduced with milk-out procedure.
Conclusion:In children with dysentery especially in presence of colicky abdominal pain, abdominal distention and no response to antibiotic therapy, abdominal ultrasound to rule out intussusception is recommended.
Key Words: Intussusception; Children; Colocolic intussusception; Abdominal distention
Introduction
Intussusception occurs when a portion of the intestine is telescoped into an adjacent intestinal segment[1]. It is very common in children all over the world, especially those under 2 years[2]. The majority of cases occur in the region of the ileocecal valve, and no lead point can be precisely identified[3]. Other types of intussusception that are rarer and have an
anatomic lead point include ileoileal, colocolic, and ileoileocolic[4]. Possible lead points include Meckel's diverticulum, polyps, neoplasms (lymphoma), and intestinal duplications[3]. Almost all cases of colocolic intussusception occur with a lead-point such as polyp or tumoral mass, a review of English-written literature showed only three cases without a lead- point[5-7].
Case presentation
A seven year-old boy with colicky abdominal pain and vomiting followed by dysentery, has been treated with metronidazole in a local health-center after positive stool for Entamobea histolytica cysts. He was sent to our hospital because of continuation of the symptoms. During the last 2 days, the symptoms worsened, his abdomen distended and his stool was totally bloody.
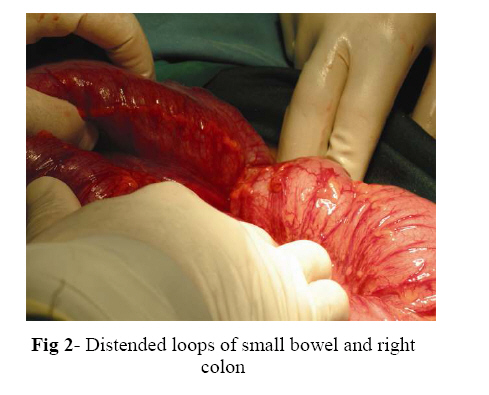
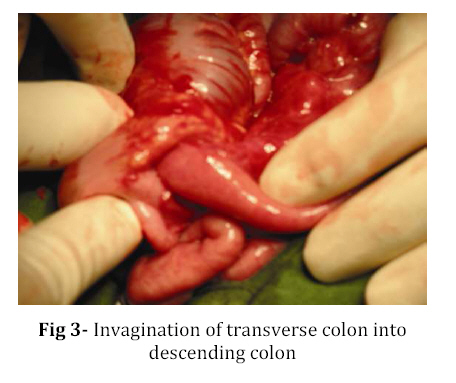
In physical examination he was conscious, febrile and severely dehydrated, BP=100/60 mmHg, PR=120/min, RR=32/min, T=38/7°C. Growth and development was normal. Head and neck were normal; breathing was normal and heart tachycardiac. Upper part of abdomen was distended and bowel sounds were hyperactive. There was diffuse abdominal tenderness without guarding or rebound. Other clinical examinations were normal. Laboratory tests were normal except for leukocytosis with left shift. Abdominal x-ray showed thick small bowel wall, multiple air-fluid levels and gasless lower abdomen (Fig 1). Pseudo-kidney appearance at splenic flexure was reported in abdominal ultrasound. After initial reduction midline laparotomy was done. Small bowel loops and right colon were severely distended (Fig 2). Invagination of lower third of transverse colon into descending colon was detected as the cause of obstruction (Fig 3) and was reduced with milking out procedure. Exact examination for underlying pathologic lead point was indeterminate. Postoperative period was unremarkable and he was discharged in good general condition. Barium enema, performed after three months, was normal and after 12 months follow up he was trouble free.
Discussion
Intussusception is the most common cause of acute intestinal obstruction in infants and young children[8]. Eighty percent of patients are younger than 24 months[1] and 95% of cases are ileocolic in location, with an equal percentage in which no pathologic lead point is evident on barium enema or laparotomy[9]. Other types of intussusception that are rarer and have an anatomic lead point occur in children older than 2 years of age[4]. Possible lead points include Meckel diverticulum[1], intestinal polyps[9-12], Peutz Jaeger[13], mucosal hematoma[14], Henoch- Schoenlein purpura[15], an inflamed appendix[16], neoplasms[17], lymphoma[1], inflammatory bowel disease [18,19], lipoma[20-23], intestinal duplications[3], hereditary angioneurotic edema[24], trauma and abdominal operation[25,26].
Colocolic intussusception in the adults is almost always a complication of pre-existing colonic disease, usually carcinoma or polypoid tumor[27].Pediatric patients presenting with documented colocolic intussusception should suggest the possibility of a colonic polyp or other mass lesion. Careful physical examination and barium studies should provide important diagnostic clues[9]. Pathologic lead point not only in laparotomy but also in three months later barium enema was not detected in our patient. He was in good condition over the postoperative period and was discharged without any medication after 5 days. He returned to clinic one month later with no complaint. Barium enema was done after three months to rule out any mislaid underlying causes for intussusception, and also after 12 months follow up he did not have any gastrointestinal problems.
Classic triad of intussusception including crampy abdominal pain, vomiting and bloody stool are seen in only 21% of patients and 70% of cases present with only 2 signs[4]. Although there were typical symptoms in our patient, progression of disease was gradual because of low level obstruction and not very young age of the patient, so that fortunately after 5 days, bowel necrosis did not happen and reduction was possible with milking out. It may be that the patient had amebial colitis at the beginning, and intussusception followed it. Intussusception can complicate specific inflammatory disease of the intestine. Occurring of it in the course of a Salmonella typhi is reported[28]. But careful examination of all regions of the intestine during laparotomy for detection of an underlying pathologic lead point such as ameboma or significant inflammation was indeterminate and the probability of amebic infection as a lead point was eliminated.
Conclusion
In children with dysentery especially with colicky abdominal pain, abdominal distention and no response to antibiotic therapy, an abdominal ultrasound should be performed to rule out intussusception.
References
- Wyllie R. Intussusception. In: Behrman RE, Kliegman RM, Jenson HB (eds). Nelson Textbook of Pediatrics. 17th ed. Philadelphia; Saunders. 2004; Pp:1242-3.
- Abantanga FA. Ileal invagination of the sigmoid colon producing a sigmoido-rectal intussusception combined with rectal prolapse in a 3-year-old child. Pediatr Surg Int.2005;21(5):400-2.
- Dominique TLM. Lower gastro-intestinal bleeding. In: Allan Walker W, Kleinman RE, Sanderson IR, et al (eds). Pediatric Gastrointestinal Disease. 4th ed. Hamilton, Ontario; BC Decker. 2004; P:273.
- Young LL. Intussusception. In: Yamamoto LG, Inaba AS, Okamoto JK, et al (eds). Case Based Pediatrics for Medical Students and Residents. Online Pediatrics Textbook. 2004. Available at: www.hawaii.edu/medicine/ pediatrics/pedtext/ Access date: Dec 2004.
- Bohrer SP. Colonic mass; an unusual adult case of colocolic intussusception in which no tumor could be identified. JAMA. 1963, 185:206-7.
- Devin R. Case of acute colocolic invagination in an adult without intestinal tumor. Marseille chirurgical. 1955;7(1): 87.
- Saidi F. Colocolic intussusception in adults due to invagination of the cecal wall. Amer J Surg.1966;112(6):927-31.
- Bines JE, Ivanoff B, Justice F, et al. Clinical case definition for the diagnosis of acute intussusception. J Pediatr Gastroenterol Nutrition. 2004;39(5):511-8.
- Arthur AL, Garvey R, Vaness DG. Colocolic intussusception in a three-year-old child caused by a colonic polyp. Connecticut Med.1990:54(9):492-4.
- Baldisserotto M, Spolidoro JV, Bahu Mda G. Graded compression sonography of the colon in the diagnosis of polyps in pediatric patients. AJR. 2002;179(1):201-5.
- Ippolito RJ, Touloukian RJ. Colocolic intussusception in an older child. Caused by a polyp of the distal colon. Clin Pediatr. 1978;17(9):720-1.
- Anwarul Haq IB, Zaheer Abassi NA. Colocolic intussusception - a rare entity in children - a case report. J Surg Pakistan. 2004;9(2):49-50.
- Howell J, Pringle K, Kirschner B, et al. Peutz-Jeghers polyps causing colocolic intussusception in infancy. J Pediatr Surg. 1981;16(1):82-4.
- Peterson CM, Menias CO, Balfe DM, et al. Adult intussusception due to cocaine-induced bowel wall hematoma: a case study. Emerg Radiol. 2006;12(4):177-9.
- Choong CK, Kimble RM, Pease P, et al. Colo-colic intussusception in Henoch-Schoenlein purpura. Pediatr Surg Int. 1998;14(3):173-4.
- Coulier B, Pestieau S, Hamels J, et al. US and CT diagnosis of complete cecocolic intussusception caused by an appendiceal mucocele. Eur Radiol. 2002;12(2):324-8.
- Ogus M, Dinckan A, Gelen T, et al. A descending colon tumour prolapsing from anus: case report. Ulus Travma AcilCerrahi Derg.2005;11(3):247-9.
- Dubinsky MC, Deslandres C, Patriquin H, et al. Pneumatosis intestinalis and colocolic intussusception complicating Crohn's disease. J Pediatr Gastroenterol Nutr. 2000; 30(1):96-8.
- Atten MJ, Attar BM, Mahkri MA, et al. Giant pseudopolyps presenting as colocolic intussusception in Crohn's colitis. Am J Gastroenterol. 1998; 93(9):1591-2.
- Downie AC, Zwirewich CV, Gray JR. Residents' corner. Answer to case of the month #54. Cecal lipoma with colocolic intussusception. Can Assoc Radiol J.1998; 49(2):132-4.
- Chan KC, Lin NH, Lien HC, et al. Intermittent intussusception caused by colonic lipoma. J Formos Med Assoc. 1998;97(1):63-5.
- Hackam DJ, Saibil F, Wilson S, et al. Laparoscopic management of intussusception caused by colonic lipomata: a case report and review of the literature. Surg Laparosc Endosc. 1996; 6(2):155-9.
- Wang TK. Adult descending colocolic intussusception caused by a large lipoma. Gastroenterol Jpn. 1992;27(3):411-3.
- Pritzker HA, Levin TL, Weinberg G. Recurrent colocolic intussusception in a child with hereditary angioneurotic edema: reduction by air enema. J Pediatr Surg.2004;39(7):1144-6.
- Zbar AP, Murphy F, Krishna SM. Adult postoperative intussusception: a rare cause of small bowel obstruction. South Med J. 2007;100(10):1042-4.
- Emil S, Shaw X, Laberge JM. Post-operative colocolic intussusception. Pediatr Surg Int. 2003;19(3):220-2.
- Figiel LS, Figiel SJ. Colocolic intussusception. AM J Dig Dis. 1963;8(12):1017-28.
- Goodall P. Intussusception in adults complicating specific inflammatory disease of intestine. Gut. 1963;4(2):132-5.
© Copyright 2008 - TUMS PUBLICATIONS
The following images related to this document are available:
Photo images
[pe08060f2.jpg]
[pe08060f1.jpg]
[pe08060f3.jpg]
| 
{kind=link}
{kind=link}
{kind=link}