 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Response of Enuretic Children with and without Hypercalciuria to Nasal Desmopressin Hamid Mohammadjafari*1, MD; Mehrnoosh Kosaryan 2, MD; Hassan Karami, MD1; Abbas Dabaghzadeh, MD1 1. Department of Pediatrics, Mazandaran University of Medical Sciences, Sari, IR Iran Received: 08/08/08; Revised: 15/11/08; Accepted: 12/12/08 Code Number: pe09001 Abstract Objective:Nocturnal enuresis is a common diagnosis in patients referred to pediatric and pediatric nephrology clinics. Nocturnal polyuria is an important patho-physiologic factor in enuresis. Hypercalciuria, with altering concentrating capacity of the kidneys, can affect children’s response to desmopressin. Key Words: Enuresis; Hypercalciuria; Desmopressin; Bedwetting; Polyuria Introduction Nocturnal enuresis (NE) is one of the most common complaints in pediatric and pediatric nephrology clinics affecting 5 to 15% of 7 year old children. The spontaneous cure rate is about 15% per year and at the age of 16 years, only 1% to 2% of children still have enuresis[1]. In spite of this high rate of spontaneous remission, NE may have a deep psychological and social impact on the affected children and their families[2-5]. Bed wetting has significant negative impacts on the self-image and performance of children[4]. On the other hand, a history of childhood bed wetting appears to increase the risk of having urinary incontinence or stress incontinence in adult life[6]. Recently, it has been documented that diurnal voiding symptoms accompany nocturnal enuresis in two-thirds of children[7]. The emerging consensus among researchers is that three major pathogenic factors are operative in NE: nocturnal polyuria, high arousal thresholds and uninhibited nocturnal detrussor contractions[8]. Relative nocturnal vasopressin deficiency with consequent polyuria is common in NE[9]. Nocturnal polyuria, albeit common, is not present in all enuretic children, but more specifically in those who respond favorably to anti-diuretic treatment with desmopressin alone or combined with anticholinergic medication[10]. In contrast to a normal diurnal rhythm with nightly increases in plasma Arginine vasopressin (AVP) levels, reduced nocturnal AVP levels have been observed in patients with primary NE[11]. Alternatively and possibly independently from nocturnal AVP levels, hypercalciuria leads to decreased Aquaporin-2 (AOP2), and expression levels has been suggested to cause primary NE[12]. The first line therapy for a sub-group of patients with enuresis associated with nocturnal polyuria and normal bladder function is desmopressin[13]. But response to this drug is unpredictable and depends on many factors. There are some controversies regarding the value of urinary calcium excretion for predicting the response[9,11]. Thus, we evaluated relation between hypecalciuria and response of enuretic children to nasal desmopressin in patients referred to pediatric nephrology clinic. Subjects and Methods It was a double blind clinical trial. Approval of the ethics committee of Mazandaran University of Medical Sciences was obtained and a written informed consent form was signed by parent/guardian prior to intervention. All patients who were presented with NE between September 2006 and March 2008 were recruited into the study. The sample size was based on the previous studies[9,11,13]. Enuresis was defined in the diagnostic and statistical manual of mental disorders- Fourth Edition (Text Revision) (DSM-IV-TR)[14]. At the initial visit all patients and their parents were interviewed about the chief complaints, present and past medical history, including voiding pattern during the day and night, bowel emptying habits, occurrence of encopresis, UTI and psycho-social or learning problems contributing to enuresis. Exclusion criteria were NE associated with day-time symptoms, urgency, frequency, urinary incontinence, urinary tract anomalies or infections, diabetes insipidus and diabetes mellitus, mental retardation, active neurological disease, abnormal urinalysis¸ use of diuretic drugs or prior enuretic therapy. All children underwent a general physical and neurological examination. At least one urinalysis was ordered for each patient. Urinary tract imaging and urodynamic studies were performed where clinically indicated. Each subject gave two urine samples in two different days and the level of urine calcium and creatinine was measured to calculate the urinary calcium/creatinine (UCa/UCr) ratio. Wet and dry nights were documented both before and after treatment by means of a voiding diary. All patients were advised to empty the bladder and restrict fluid and fruit intake prior to going to bed. Patients were initially given 10 micgr nasal desmopressin and the dose was increased gradually to a maximum of 40 micgr, if they still had more than 1 wet night per week. A primary outcome measure was the mean number of wet nights per week during a 2 week observation period without treatment and after 6 weeks of therapy. Detailed voiding diaries were maintained by the patients and/or their parents throughout the study to make notes on enuretic events. The children in the study were consequently classified as:
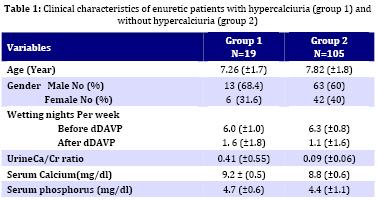
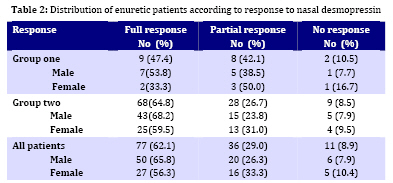
Patients were divided into hypercalciuric and non hypercalciuric groups on the basis of urinary calcium level. Plasma calcium, phosphprus, and alkaline phosphatase levels were measured in all hypercalciuric children and only idiopathic hypercalciuric cases were included. The state of UCa/UCr was blind for children's parents and the clinician who prescribed the nasal vasopressin and monitored the responsiveness of the patients. After the study period, the group affiliation of patients based on the UCa/UCr was opened. Statistical evaluation was performed with SPSS 11.5 version for Windows and the results were analyzed by Chi-square. P<0.05 was considered significant. Findings One hundred and twenty four children were involved in the study within two groups: group 1 (n=19) consisting of hypercalciuric enuretic patients, and group 2 (n=105) consisting of non hypercalciuric enuretic patients. There were no statistical significant differences between groups according to age, sex and mean wetting nights per week. Table 1 shows the baseline characteristics of the groups. The age of patients ranged between 6 and 12 years of age (mean7.7 ±1.8) and 76 (61%) of them were boys. Mean of wet nights was 6.0 and 6.3 in group 1 and group 2 respectively. After 4 to 6 weeks of desmopressin therapy, a full response was observed in 77 (62.1%) children. Full response was observed in 47.4% of group 1 and 64.8% of group 2 patients and this difference was statistically significant (P<0.04). Table 2 shows the response of children to desmopressin. In group 1, among 9 full responders, six patients responded to 10 and another three to 20 mcg desmopressin/night. In second group, 14, 3 and 1 patients had full response to 10, 20, 30 and 40 mcg/night of desmopressin respectively. No serious adverse events were observed. One patient had an episode of a febrile seizure; however, serum electrolytes revealed no abnormalities and EEG confirmed epilepsy. Night terror and nasal irritation were developed in 2 and 5 patients respectively. Discussion Despite extensive multidisciplinary investigations we know very little about nocturnal enuresis. Although there are many treatment modalities, pharmacotherapy is the most popular choice. In our prospective study we showed that 15.3% of enuretic patients have hypercalciuria. We found that the overall full and partial responses to nasal desmopressin are 62.1% and 29% respectively. There were no statistical significant differences between hyper-calciuric and non-hypercalciuric groups according to age, sex and mean wetting nights per week. The view that hypercalciuria is an important pathogenic factor in enuresis was first proposed by Pace et al who noted that a proportion of enuretic children had absorptive hypercalciuria[16]. In our study, 15.3% of enuretic patients had hyper- calciuria that was more than in healthy children. Safarinejad demonstrated that the prevalence of hypercalciuria is 1% in healthy Iranian children, and 95th percentile value for Ca/cr ratio is equal to 0.12 for 7-10 and 0.115 for 11-15 year-old children[15]. Pace et al reported that only 21 of 406 enuretic children had increased urinary calcium excretion[16]. Conversely, Aceto found that nocturnal hypercalciuria was present in 39.8% of patients[18]. On theoretical grounds, one would suspect that children with hypercalciuria would respond to desmopressin poorly because hypercalciuria independently from nocturnal enuresis could lead to decreased Aquaporin-2 expression levels and nocturnal polyuria[11]. In addition, Aceto mentioned that nocturnal hypercalciuria has a pivotal role in nocturnal enuresis, as it is significantly associated with low ADH levels and nocturnal polyuria. A new classification of nocturnal enuresis subtypes based on calciuria, is mandatory to address treatment properly[18]. The daily dose of dDAVP produced a significant decrease in the number of wet nights. The full response achieved with nasal desmopressin was 62.1%. This response rate was comparable to other studies. According to our experience, and those published in the literature[19], the overall success rate of desmopressin treatment ranged from 35% to 65%. Recently Ferrari et al performed a study on 50 enuretic children who received dDAVP (0.2 mg orally at bed time) and found 50 and 51 children who received homotoxicological remedies and placebo respectively. There was a significant (62.9%) decrease in wet nights in dDAVP group, compared with the other two groups[20]. In a Chinese study, 52% of children responded to oral dDAVP (0.4 mg)[21]. The mean bed wetting nights decreased significantly in some other studies[22,23]. We noted a lower incidence of full response to dDAVP in hypercalciuric than non- hypercalciuric enuretic children (47.4% vs. 64.8%). Therefore, according to our result, hypercalciuria acts as a frequent pathogenetic factor and appears to be responsible for poor treatment responses. Neveus et al performed a study on 28 enuretic children who were (diuresis dependent) and 15 who were not (non-diuresis dependent) responsive to desmopressin therapy[9]. No differences were found concerning urine osmolarity and calcium urinary excretion between the two groups and a group of 51 dry controls. Pace et al studied 406 patients with primary monosymptomatic nocturnal enuresis[16]. They found that in 21 patients with persistent enuresis, the urinary calcium to creatinine ratio was significantly high. They were given an appropriate diet. After 3 months, NE had ceased completely in 4 patients (19%), five patients improved with oxybutinyne and 12 remaining children received dDAVP. Both calciuria and enuresis ceased in all 12 patients. As other clinical studies, our study has a few limitations. For diagnosis of hypercalciuria, we have checked random urine samples in terms of the UCa/UCr ratio. The measurement of 24-hr urinary Ca is more reliable than the random urine sampling, but in NE children who wet their bed, it would be very difficult to collect the urine accurately for 24 hours. To decrease this limitation, we have analyzed two separate morning urine samles to determine the UCa/UCr ratio. Conclusion Based on the results of this study, hypercalciuria affects the responsiveness of patients to desmopressin in primary NE. Hypercalciuria should be evaluated in NE children and hypercalciuric patients may need the higher initial doses of desmopressin. Acknowledgment This study was supported by Thalassemia research center of Mazandaran University of Medical Sciences. The authors gratefully acknowledge the many people on the staff at Boalisina Hospital who contributed to theinvestigation and care of the patients studied, especially colleagues in the research center. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences,All rights reserved. The following images related to this document are available:Photo images[pe09001t2.jpg] [pe09001t1.jpg] |
| |||||||||

{kind=link}
{kind=link}