 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
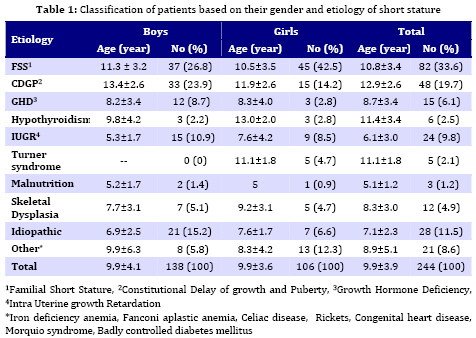
Iranian Journal of Pediatrics, Vol. 19, No. 1, March, 2009, pp. 35-39 Etiology of Short Stature in East Azerbaijan, Iran Siamak Shiva*1, MD; Alireza Nikzad1, MD 1. Department of Pediatrics, Tabriz University of Medical Sciences, IR Iran Received: 11/06/07; Revised: 05/11/07; Accepted: 27/12/07 Code Number: pe09005 Abstract Objective: Short stature is a common problem encountered by pediatricians and is the most common cause for referral to pediatric endocrinologists. Although most children referred with short stature are normal and classified as normal variants of stature (constitutional growth delay and familial short stature), it may sometimes be the only obvious manifestation of an endocrine or systemic disease. The objective of this study was to assess the characteristics of patients referred to pediatric endocrinology clinic because of short stature and determination of the etiology. Key Words: Short stature; Etiology; Children; Familial; Constitutional Introduction Short stature (SS), defined as a height of more than two standard deviations below the average for same age and sex, is one of the most common causes of referrals to pediatric endocrinologists[1,2]. The way by which the short stature influences the psychosocial and educational function of short children is controversial[3,4]. Likewise, there is no compelling evidence to show an association between short stature and cognitive and psychosocial maladaptation or dysfunction[5]. Nowadays, because of the widespread use of growth hormone in treatment of these patients, the parents do not accept the shortness of their children at all[6]. This resulted in increasing of referrals for height augmentation. Many of the patients referred with SS have no identifiable medical abnormality and are classified as constitutional delay of growth and puberty (CDGP), familial short stature (FSS), or idiopathic short stature (ISS). However, in some cases it may be the only clinical manifestation of a systemic or endocrine disorder[1,7,8,9]. A careful and detailed clinical evaluation helps us to differentiate pathologic forms from normal variants, and prevents unnecessary evaluations, wasting time and expenses[9]. Based on the mentioned matters, many endocrine centers in this country[10,11,12], and throughout the world[2,13,14,15], attempted to investigate the etiology of SS in their areas. Therefore, we decided to evaluate the subjects referred with complaint of SS and to determine its causes in our area (province of East Azerbaijan/ Iran). Subjects and Methods This descriptive-analytic and prospective study was carried out between July 2005 and December 2006. All of the subjects referred to outpatient pediatric endocrinology clinic of Tabriz University of Medical Sciences with complaint of SS were recruited. Subjects that haven't completed at least 6 months follow up visit were excluded. At first a complete medical and growth history was taken and a thorough physical examination carried out. Seca balance and studiometer were used for weight and height measurements. National Center for Health Statistics(NCHS) growth charts were used for calculation of height Standard Deviation Score (SDS). No paraclinical study was undertaken on subjects that were referred after completing their puberty and had no abnormal finding on their clinical examination. Patients with normal physical examination and body height less than 2SDS below mean were followed only for their growth velocity and no laboratory test was done on them at beginning. Patients with a body height more than 2SDS below mean for same sex and age, underwent complete paraclinical evaluation including: wrist and hand X-ray for assigning bone age, ESR, CBC, serum creatinine level, arterial blood gases, serum electrolytes and alkaline phosphate, stool examination and Sudan test, urine analysis and culture, thyroid function tests, anti gliadin and anti endomyseal antibodies. Patients with normal laboratory findings and growth velocity lower than 25% normal growth rate for the same sex and age, and also those with a body height more than 3SDS below mean, underwent GH provocative test. This test was carried out with clonidine and, if needed, the patients underwent a second test with methyl dopa. In peripubertal patients the suitable sex steroids were used for priming before test. GH provocative tests were done following an overnight fast. In short girls when the etiology of their shortness was unclear, chromosomal analysis ordered. Bone survey was done when skeletal dysplasias were suspected. Finally after complete evaluation and suitable treatments (if needed), subjects who completed at least 6 months follow up were classified as: 1) Those who were not really short (body height less than 2SDS below mean and height velocity greater than 25%). 2) Those who were short (body height more than 2SDS below mean for same sex and age). The short patients were classified as following: 1) FSS (skeletal age proportional with chronologic age, short parents and no abnormal paraclinical findings), 2) CDGP (shortness with normal growth rate, retarded skeletal age, positive family history of constitutional growth delay, delayed puberty in patients who were in pubertal age), 3) GH deficiency (severe SS, delayed skeletal maturation, low growth velocity, maximum GH level less than 10 ng/ml in two provocative tests with normal findings in all other laboratory tests), 4) Hypothyroidism, 5) Turner syndrome (based on karyotype), 6) Skeletal dysplasia (according to bone survey), 7) IUGR (intra uterine growth retardation with no appropriate growth rate after delivery), 8) Malnutrition, 9) ISS (shortness and delayed bone age with completely normal clinical and paraclinical findings and no abnormality in growth hormone study, 10) Other causes. After gathering and classifying initial data, we used SPSS software version 12 for statistical analysis. T-test, Chi-Square, NPar Chi-Square statistical tests were used. Continuous data were presented as mean±SD and categorical data were presented as proportions. P-values less than 0.05 were considered statistically significant. According to the fact that all studies and therapies were based on patients, needs and we refused any unnecessary examinations and their private data will not be obtained by any factual or legal authorities, this research does not have any ethical problems. Findings During 18 months, 482 subjects were referred with complaint of SS. One-hundred and three of them were excluded because they did not complete at least 6 months follow up and 379 children and adolescents that were followed about 6-18 (mean 6.8±2.3) months, containing 192 (50.7%) boys and 187 (49.3%) girls, entered the final analysis. There was no statistically meaningful difference between the number of referred boys and girls (P=0.066). The patients were between 2-23 years of age (mean 9.7±3.7), and 34.8% (132 cases) of them were not provable short and only 65.2% (247 cases) were really short (height more than 2SDS below mean). The difference between referred short boys (71.9%) and girls (58.3%) was significant (P=0.006). 28 (15%) of 187 studied girls had experienced their first menstrual period at least six months before their referral. The mean height SDS of short patients was -4±1.24 which was -3.45±1.15 for short boys and -3.45±1.35 for short girls, the difference was not statistically meaningful (P=0.5). Three of 247 short subjects were not paraclinically evaluated because they were referred after their first menstruation. Remaining 244 short subjects underwent complete examinations. The Table 1 shows number and mean age of the patients based on their final diagnosis. No statistically meaningful difference (P=0.8) was observed between the age of short boys (9.9±4.1 years) and short girls (9.9±3.6 years). Most of short boys (50.7%) and short girls (56.7%) had non-pathologic types of SS (FSS or CDGP), the difference was not significant (P=0.8). Totally 53.3% of cases were due to non-pathologic types of SS. In this group, 63.1% were due to familial SS and 36.9% to CDGP. The main etiology of non-pathologic SS was FSS in girls and in boys. In patients with growth hormone deficiency, the maximum response of GH to provocative tests was 5.4 ng/ml. Discussion Short stature is a common finding among general population and between 0.1% and 2.5% of people in different areas have a body height more than 2SDS below mean[3]. Also the most common cause for referrals to pediatric endocrinology clinics is SS, but in many of these patients there is no pathologic reason for their shortness[1]. In our study most of short patients (53.3%) were placed in non- pathologic group (FSS or CDGP) too, and in 11.5% of cases no pathologic cause was found. In addition, our study showed that most of the subjects with complaint of SS were not short at all. This point indicates that they haven’t been examined properly before referral to us. Researches in other parts of the world have indicated that most cases of SS are related to non-pathologic causes[2,13,16]. In researches that have been carried out in this country, in most cases there were no identifiable medical reasons for shortness and have been related to FSS or CDGP[10,11]. In our study there were no significant differences between numbers of two sexes, their ages at referral time, and their height SDS. But the portion of subjects that were not really short was higher in females than in males and most of females were referred after puberty. It seems that in our society girls prefer to be tall but their parents do not have enough information about SS and steps of normal growth. Psychosocial adaptation and degree of parents' awareness are critical determinants in seeking for evaluation and treatment of SS[17]. As in the study of Bhadada and his colleagues, in our study also the most common cause of SS in females was FSS. Another noticeable reason for SS in our study was children who were born with IUGR and did not have appropriate growth rate after delivery. It is important to know that the SS is a common complication in children born with IUGR[14]. These children have sevenfold greater risk of being short and 8% of them will have adult height less than -2SDS, which corresponds to 20% of short adult population[18]. Most of these children gain suitable catch up growth by two years of age but if they cannot reach proper growth rate till three years of age, they will need a vast and precise evaluation[19]. In spite of other researches that have reported the incidence of GH deficiency (GHD) between 16% and 32% among short subjects in Iran [10,11,12], the rate of GHD was not considerable (6.1%) among our short patients. Most of foreign references believe that GHD is an uncommon cause of SS and according to researches that have been carried out in different parts of the world, the incidence of idiopathic GHD is about 1/3500 to 1/4000[9,20]. It should be considered that the research center situation, manner of the patient selection, quality of GH provocative with or without priming with sexual steroids, are important in determination of GHD. In this research we used GH provocative tests for patients with a body height more than 3SDS below mean, delayed skeletal maturation and growth velocity less than 25% in at least 6 months follow up. It seems that most of Turner cases diagnosed in endocrinology clinics were above ten years of age[21,22] when they were referred because of SS or delayed puberty. It was true in our study too. The main limitation of our study was that a great number of our patients haven’t completed the six months follow-up and were eliminated from the final analysis. Conclusion A significant proportion of subjects referred with complaint of short stature to pediatric endocrinology clinics are not really short (height above -2SDS), and have suitable growth velocity. In more than 50% of short subjects no pathologic cause was found, and GHD is not a common cause of short stature. Acknowledgment The authors acknowledge the research vice chancellor office of Tabriz University of Medical Sciences for support of this study and so Miss Rahimzadeh for her cooperation in editing this article. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences,All rights reserved. The following images related to this document are available:Photo images[pe09005t1.jpg] |
| |||||||||

{kind=link}