 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
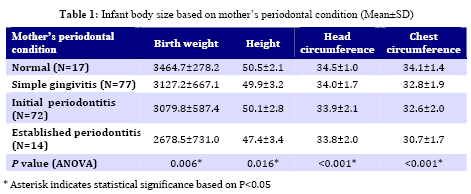
Iranian Journal of Pediatrics, Vol. 19, No. 2, June, 2009, pp. 101-107 Relationship between Maternal Periodontal Condition and Body Size of Newborns Adileh Shirmohammadi1, DMD; Reza Pourabbas*1, DMD; Naemat Bilan2, MD; Mohammad-Taghi Chitsazi1, DMD 1. Department of Periodontics, Tabriz University (Medical Sciences), Tabriz, IR Iran Received: Oct 05, 2008; Final Revision: Dec 12, 2008; Accepted: Jan 25, 2009 Code Number: pe09016 Abstract Objective:It has been suggested that periodontal disease may be a risk factor for a number of multifactorial systemic conditions such as preterm deliveries. The aim of the present study was to examine the relationship between maternal periodontal disease and body size of newborns. Key Words:Newborn; Periodontal disease; Body size; Preterm; Low birth weight Introduction Systemic maternal infections are hypothesized to increase the risk of placental infections, Premature rupture of membranes, premature labor and preterm birth by release of inflammatory cytokines and increased prostaglandin production[1,2]. Periodontal disease is a chronic, low-grade, gram-negative anaerobic infection of periodontal tissues that is associated with an increase in the systemic levels of inflammatory cytokines[3]. Periodontal organisms have been isolated from the amniotic fluid, suggesting the possibility of hematogenous spread [4,5]. Periodontal disease could potentially influence pregnancy outcomes through indirect mechanisms involving inflammatory cytokines or direct translocation of bacteria and its products to the feto-placental unit. Previous epidemiologic studies have reported positive associations between periodontal disease and adverse pregnancy outcomes, including preterm low birth weight [6,7], low birth weight [7,8], preterm birth[9], fetal growth restriction[10], and preeclampsia[11]. Body size (weight, height, and head and chest circumference) at birth are important clinical indicators widely used for evaluation of prenatal growth [12]. Although a large number of studies have evaluated the effect of periodontal disease on premature child birth, no studies have, so far, focused on the influence of this chronic disease on the developmental status of newborns. Therefore, the present study was undertaken to determine the influence of periodontal disease in pregnant women on the body size of their newborn babies. The main objective of the present study was to evaluate a hypothesis: Periodontal disease in pregnant women can have a detrimental effect on intrauterine development of babies. In case of an association between these two, future studies can evaluate this hypothesis. Subjects and Methods The present study was an analytical/cross-sectional study (correlational type). The study population consisted of pregnant women aged 17 to 40, who had referred to the Alzahra Hospital of Tabriz University (Medical Sciences) between June and August 2007. Exclusion criteria included systemic conditions such as severe anemia, diabetes, cardiovascular disorders, hepatic deficiency, high blood pressure, venereal disease, urinary infections, bacterial vaginitis, and viral infections or environmental factors such as tobacco use, alcoholism, narcotic drug use, x-rays during the first semester, anti-convulsive drugs, associated premature birth or intrauterine growth delay and an obstetric history which included multiple pregnancies, more than 3 deliveries, severe polyhydramnios and oligohydramnios, umbilical cord coiling, women who did not present for regular prenatal checkups, i.e. fewer than 5 consultations and finally women who had opted for Cesarean section before the onset of labor pains. A total of 180 women met the criteria for participation in the studyand a census procedure carried out in order to acquire and record the data from the subjects during the period of study. The study design was approved by the Ethics Committee and supported by the Pediatric Research Deputy of Tabriz University (Medical Sciences). The nature of this investigation was explained to the patients in detail and the patients signed an informed consent form. All data were collected within 48 hours after delivery. Clinical histories taken by the attending obstetrician (factors associated with premature birth or intrauterine growth delay) were reviewed by one of the authors to ensure that none of the afore-mentioned exclusion criteria was present. Measurements were taken by one examiner trained in the technique. After delivery, classification was carried out on the basis of gingival and plaque indices (Ainamo & Bey)[13] and mean of attachment loss. In this index, bleeding from the gingival margin and visible plaque have a score of “1”, while absence of bleeding and no visible plaque have a score of “0”. Attachment loss was measured with a Williams periodontal probe (PWD, Hu-Friedy Immunity, USA) for all the existing teeth on four surfaces (buccal, mesial, distal, and palatal or lingual) and the means were calculated. Based on the results the pregnant women were divided into 4 groups as follows: Group 1: Normal with no gingival inflammation (GPI=0) and no attachment loss. Group 2: Simple gingivitis with gingival inflammation (GPI=1) and no attachment loss. Group 3: Initial periodontitis with gingival inflammation (GPI=1) and attachment loss of <2 mm. Group 4: Established periodontitis with gingival inflammation (GPI=1) and attachment loss of >2 mm. Measurements relating to birth weight by gr, newborn length by cm, and head and chest circumference by cm were retrieved from the newborns' medical files. Means of these variables were calculated for each group and compared using one-way ANOVA. If there were statistically significant differences between the groups, post hoc tests were used for further analysis. A P-value of <0.05 was considered significant. Since various factors can influence developmental parameters an effort was made to control other known risk factors and omit confounding parameters using regression analyses. These confounding factors included age, weight, height and the educational status (defined as the years of school attendance) of mothers, the economic status of the family (defined as poor, moderate, and good), the number of pregnancies, newborn gender, and fathers' height and age[12,14,15,16]. Findings The subjects in the present study consisted of 180 mothers aged 17-40 years with a mean age of 26.5 (±4.6) years. Means of mothers' weight and height were 64.1 (±11.9) kg and 160.5 (±8.0) cm, respectively. The mean of mothers' school attendance years was 7.9 (±5.1). A total of 70 (69%) of mothers came from poor families, 74 (41.1%) had moderate economic status, and 36 (20.0%) came from affluent families. A total of 91 (50.6%) of mothers were experiencing their first pregnancy, 56 (31.1%) were having their second pregnancy and 33 (18.4%) were experiencing their third pregnancy. A total of 157 (87.2%) mothers had no history of abortion/miscarriage, 16 (8.9%) mothers had one abortion/miscarriage experience in their history and 7 (3.9%) had 2 cases of abortion/miscarriage in their medical history. Evaluation of mothers' periodontal status revealed that 17 (9.4%) mothers had normal periodontium, 77 (42.8%) had simple gingivitis, 72 (40.0%) had initial periodontitis, and 14 (7.8%) suffered from established periodontitis. Means of fathers' height and age were 174.3 (±12.6) cm and 30.8 ± 6.4 years, respectively. Baby girls and baby boys comprised 80 (44%) and 100 (55%) of the newborns. A total of 172 (95.6%) of the babies were carried to full term and 8 (4.4%) were born preterm, one of whom was born of a mother with simple gingivitis, three were born of mothers with initial periodontitis and four were born of mothers with established periodontitis. Statistical analysis using one-way ANOVA demonstrated statistically significant associations between the weight, head and chest circumference, and height at birth and the periodontal status of mothers from healthy and normal periodontium to gingivitis, to initial periodontitis, and to established periodontitis (Table 1). Multiple regression analyses revealed that of all the variables involved only the following variables had associations with weight at birth, respectively:
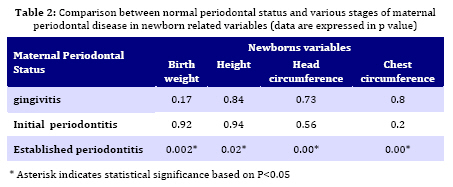
The correlation coefficient (R=0.52) for those variables was highly significant (P<0.001). It is noteworthy that mothers' periodontal status had the strongest influence on gestational age at birth (P=0.22, R=0.17), followed by mothers’ educational status (P=0. 22) and the number of pregnancies (P=0.006). A post hoc Tukey test revealed that there was only a statistically significant difference between the periodontal health and established periodontitis, i.e. periodontaldisease in mild forms (gingivitis) and initial periodontitis do not influence these variables and only the severe form of the disease influences the variables (Table 2). Multiple regression analyses indicated that mothers' periodontal status and fathers' age had an independent correlation with the newborns' head circumference (P =0.001, R = 0.25). Newborns' chest circumference had the strongest correlation with the following variables, respectively, and other variables had no influence on it (P<0.001, R=0.3):
Newborns' length at birth had the strongest correlation with the number of pregnancies and mothers' periodontal status and other variables did not demonstrate any correlation:
Discussion This research examined the relationship between maternal periodontal disease and the body size of the newborn infants after controlling for the traditional risk factors for premature child birth and low birth weight. The average birth weight decreased as the severity of mother's periodontal disease increased. In addition, a strong association was observed between maternal periodontal disease and preterm birth. These results are consistent with those reported by Collins et al, who suggested that infection with Gram-negative periodontal pathogens might induce adverse effects on the fetus, depending on the degree of infection[17]. Offenbacher et al had similar results when they measured the attributable risk of periodontal disease in pregnant women after controlling for traditional risk factors. A study by Pitiphat et al showed that periodontitis is an independent risk factor for poor pregnancy outcome among middle-class women[18]. Radnai et al showed that the average weight of newborns of mothers with periodontitis was significantly less than that of women without periodontitis[19]. What distinguishes the present study from other studies on the subject is the evaluation of developmental parameters in newborns whose mothers suffered from varying degrees of periodontal disease. Since a number of factors can influence these parameters[12,14-16] an effort was made to control other known risk factors and eliminate confounding parameters using regression analysis. This test indicated that the greatest independent correlation existed between head circumference and maternal periodontal status. This relationship might be attributed to the effect of chronic infections on nervous system development. Animal studies have demonstrated the influence of chronic infections on nervous system development in infants[20]. Of the variables evaluated, chest circumference had the strongest correlation with maternal periodontal status. Evaluation of newborns' length demonstrated that, second to the number of pregnancies, it had the strongest correlation with maternal periodontal status. Although no explanation can be found in the references available, the effect of chronic infections on skeletal system development has been documented in animals[20]. The results showed that number of pregnancies, mother's educational status, mother's weight, and mother's periodontal status can influence weight of the newborn, are consistent with the results of related articles. The study of Gazolla et al showed that educational level, previous preterm birth, and periodontal disease were related significantly to preterm delivery[21]. There was only a statistically significant difference between the periodontal health and established periodontitis, but the study of Vettore et al revealed that periodontal disease was not more severe in women with preterm low birth weight babies [22]. It should be pointed out that the present study was carried out to establish an association between height, and head and chest circumference in newborns with maternal periodontal disease and this disease cannot be considered a causative agent. It is important to consider the possibility that there is some underlying mechanism causing both periodontal disease and pregnancy outcomes. Impaired immune system can be mentioned as an example. Some authors suggest that the response of peripheral blood monocytes to lipopoly-saccarides [LPS) from various sources may vary in individuals from the same population[23]. This implies that some individuals experience an abnormal inflammatory response to bacterial LPS, resulting in high levels of mediators such as prostaglandin E2, interleukin-1β, and TNF-α[23,24]. This situation may contribute to an increase in periodontal disease severity, preterm labor, and low birth weight in some women. Cross sectional studies have their own limitations and at the present study, although the periodontal indices evaluating the gingival inflammation (such as Ainamo- Bey, Loe & Sillness etc.) showed the mothers periodontal condition shortly after delivery, it does not provide reliable information on previous disease activity (in normal and simple gingivitis groups). The present study indicated that the periodontal disease of pregnant women was associated with infant body size. In order to improve oral hygiene and periodontal status there is a need to develop preventive programs for pregnant women in coordination with the gynecological and dental professions. Periodontal therapy is able to reduce pregnancy adverse[25] and it would be an essential to prevent future complications among pregnant women particularly those with periodontitis. Conclusion The present study demonstrated that the strongest association was observed between maternal periodontal status with infant body size (length, and head and chest circumference). It is noteworthy that longitudinal studies are required to substantiate this association. Acknowledgment This study was supported by a grant and approved by the ethics committee of research of Tabriz University (Medical Sciences). References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences,All rights reserved. The following images related to this document are available:Photo images[pe09016t2.jpg] [pe09016t1.jpg] |
| |||||||||

{kind=link}
{kind=link}