 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
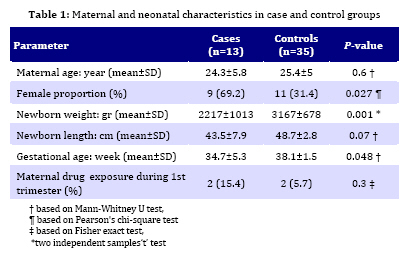
Iranian Journal of Pediatrics, Vol. 19, No. 2, June, 2009, pp. 130-134 Serum Copper Concentration in Newborns with Neural Tube Defects in Northern Iran; A Case Control Study Mohammad-Jafar Golalipour*1, PhD; Azad-Reza Mansourian2, PhD; Abbas-Ali Keshtkar3, MD, PhD 1. Department of Embryology and Gorgan Congenital Malformations Research Center, Gorgan University of Medical Sciences, Gorgan, IR Iran Received: Sep 25, 2008; Final Revision: Nov 03, 2008; Accepted: Feb 02, 2009 Code Number: pe09020 Abstract Objective:This study was conducted to determine the eventual association between copper deficiency in newborns with neural tube defects (NTD) in Northern Iran. A high prevalence of neural tube defects has been reported from this region. Key Words: Neural tube defects; Spina bifida; Anencephaly; Copper; Newborns; Iran Introduction Neural tube defects (NTDs) are an important cause of infant mortality and childhood morbidity [1, 2]. Several studies revealed a high incidence of NTDs in Iran. NTDs occur in Iran about 28-32 per 10000 births in Iran[3,4]. This rate is higher than the incidence of NTDs in United States (9.3 to 14.6/10000)[5], England (17.9/10000)[6] and France[7]. Etiology of NTD is considered multifactorial, with genetic, environmental and nutritional factors playing some role[8,9,10]. There is some evidence to suggest that the incidence of NTDs could be reduced even further by larger folic acid supplements, there may be other environmental factors, probably nutritional, that contribute to the etiology of NTDs, because folic acid supplementation and fortification of food with folic acid did not eliminate all NTDs[11,12,13]. There is considerable inconsistency concerning the relationship between plasma copper (Cu) concentrations and the occurrence of NTDs. Whereas O'Shea et al reported that exposure to copper sulfate resulted in a failure of development of NTDs in mouse embryo[14] and Graham et al showed that copper–bearing intrauterine devices were related with anencephaly in anecdotal cases[15], Keen et al reported that copper deficiency rather than the excess copper was related with teratogenesis[16]. Besides, a study in Denmark found no relation between copper concentration of serum and occurrence of NTDs[17] . Copper plays key role in embryonic and fetal development and copper deficiency during this period of life may be followed by fetal brain anomalies. The reasons behind the teratogenicity of copper deficiency are due to reduced superoxidase dismutase enzymatic activity and the elevation of reactive oxygen species with ultimate oxidative damage [16,18,19]. Thus, regarding a lack of documented report on this, we conducted this study to look for an association between serum copper level and neural tube defects in newborns in Northern Iran, where a high prevalence of neural tube defects has been reported. Subjects and Methods This hospital based case control study was conducted during 2005-2006 at the Dezyani hospital in Gorgan located in the north of Iran. The study was approved by the Human Research Committee at the Gorgan University of Medical Sciences. The cases and control group were 13 and 35 newborns with NTDs and healthy subjects, respectively. The control were chosen from the hospital delivery list following the NTDs subjects were born. Control to case ratio was almost 3:1. All babies delivered in this hospital during the investigation period were examined after delivery with NTD by a gynecologist and later the diagnosis was confirmed by a pediatrician. The health of newborns in the control group was assessed clinically by a gynecologist and pediatrician. A questionnaire covering all relevant clinical and demographic factors was filled out for each case and control infant by the pediatrician and then completed by a nurse during an interview with the mothers. The data included: birth date, sex, birth weight, length, gestational age and type of NTD. Also recorded were: mother’s age, mother’s parity, and mother’s history of exposure to drugs during the 1st trimester.Anthropometric measures of the newborn were recorded as per standard techniques. Peripheral blood sample was collected from case and control groups maximum two hours after deliveryfor copper measurements. Serum was separated and analyzed for copper level by spectrophotometric method, using Randox Kit UR. Copper levels between 12-24.4 μmol/l were considered as normal and individuals with serum copper level less than 12 μmol/l were labeled copper deficient. Categorical data were compared by Chi-square and Fisher’s exact test. Mann Whitney U test and unpaired Student’s t test were used for comparison of mean values. Presence of neural tube defect was considered as the dependent factor in multivariable logistics regression analysis. Independent factors included in the analysis were parity, history of abortions, maternal drug exposure and copper deficiency as dichotomous variables. Data were analyzed using SPSS 11.5 and STATA SE/8.P<0.05 was the criterion for a significant difference. Findings Baseline characteristics of the two groups are depicted in Table 1. However, control group babies were heavier and lengthy as compared to those of the study group. The gestational age of NTDs was less than controls. Serum copper level (mean±SD) in newborns with NTD and healthy normal newborns was 16.5 (±7.2) μmol/l and 16.7 (±6.6) μmol/l, respectively. In case group 38.5% of newborns and in control group 28.6% of infants had copper deficiency. Logistic regression analysis showed no association between the presence of NTD and copper deficiency (OR:1.6, 95%CI=0.3-7.1, P=0.5). Discussion This study indicated that 38.5% of newborns in case group and 28.6% in control group had copper deficiency. Logistic regression analysis showed no association between the presence of NTD and copper deficiency. This finding is similar to results from Macmichel study in Australia [20]. Macmichel et al reported that there was no association between NTD and copper deficiency in a case–control study in Australia. On the other hand, Cengiz et al in Turkey[13], Buamah et al in England [21] and Morton et al in South Wales[22] reported that there is a relation between copper concentration and NTD. Morton et al[22] reported a significant correlation between low copper in drinking water and the occurrence of neural tube defects in South Wales, with the implication that a primary deficiency of copper could result in birth defects in humans. Also Buamah et al [21] observed that low serum copper concentrations in pregnant women were associated with an increased risk for anencephaly. Cengiz et al[13] reported that high serum copper concentrations in pregnant women were associated with an increased risk for neural tube defects. Most studies reporting a relation between copper concentration and NTDs were based on the maternal copper status; studies using newborn serum are limited. Bro et al in Denmark [17]] reported that there is no relation between copper and NTD. Bro reported that copper concentrations in malformed infants did not differ from concentrations in reference infants. The findings of Bro study are similar to the results of our study. Evidence about copper in prenatal development and pregnancy is controversial. O'shea and Kufman[14] reported that exposure to copper sulfate generally resulted in the failure of elevation of the neural folds and consequent development of NTDs in mouse embryos. Except for some anecdotal cases of fetal NTDs in pregnant women with a Copper intrauterine device in place[15], there are no consistent reports of abnormalities in the offspring of mothers with untreated Wilson's disease, which is usually characterized with spontaneous abortions[16]. Saner and Yuksel[23] reported that maternal serum copper levels were significantly higher in NTD pregnancies than healthy controls in which serum and hair zinc levels were significantly low. Our pervious study[24] indicated that newborns with NTDs had zinc deficiency in comparison with healthy newborns. In recent study we did not measure serum zinc level, but one possible mechanism can be related to zinc-copper interactions during intestinal absorption which could be the answer for the relative increase of Copper in patients with NTDs. The anti-copper mechanism of zinc action is unique, it induces intestinal cell metallothionein, which binds Copper and prevents its transfer into blood. As intestinal cells die and slough, the contained Copper is eliminated in the stool. Thus, zinc prevents the intestinal absorption of copper[25]. A reversed mechanism (increased absorption) in a zinc deficient woman may be responsible for increased copper levels. Hurley study[26] showed that teratogenesis resulting from trace elements can occur as a result of transient deficiency of zinc, selenium, and copper if it occurs at a critical time before the neural tube formation. However, this study has certain limitation. Firstly, the case and control groups are not age and sex matched. Also, this study had sample size limitation which leads to low statistical tests power. We suggest that similar studies be conducted with larger sample size. We recommend conducting a cohort study for assessing the relationship between serum copper and zinc. Conclusion This case control study which was done on 13 affected NTD newborns and 35 normal healthy newborns in Gorgan, northern Iran, showed that there isno association between the presence of NTD and copper deficiency. Acknowledgment The authors thank the research deputy of Gorgan University of Medical Sciences for the financial support. The authors also wish to thank the director, the manager, the infant ward of Dezyani hospital, and Mrs. Hajizade for their assistance. Special thanks also go to Dr Arezo Mirfazeli the neonatologist of Dezyani hospital. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09020t1.jpg] |
| |||||||||

{kind=link}