 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
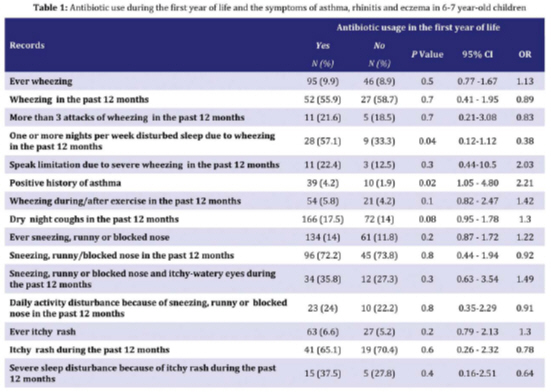
Iranian Journal of Pediatrics, Vol. 19, No. 2, June, 2009, pp. 141-146 Antibiotic Use and Symptoms of Asthma, Allergic Rhinitis and Eczema in Children Mehran Karimi1, MD;Mohsen Mirzaei2, MD, MPH 1. Department of Pediatrics, Shahid Sadoughi University of Medical Sciences, Yazd, Iran Received: Sep 25, 2008; Final Revision: Nov 03, 2008; Accepted: Feb 19, 2009 Code Number: pe09022 Abstract Objective: Allergic diseases are frequent in children and their prevalence and severity differ in different regions of the world. It has been hypothesized that antibiotic use, earlyin life, may increase the subsequent risk of asthma and other allergic disorders. The aim of this study was to investigate the association between the use of antibiotics in the first year of life and the subsequent development of asthma and other allergic symptoms. IranianJournal of Pediatrics, Volume 19 (Number 2), June 2009, pp. Pages: Key Words: Allergy; Antibiotics; Childhood asthma; ISAAC Introduction Antibiotics are commonly used to treat infections during earlychildhood.Over the past four decades, there has been a significant increasein allergy and asthma in some countries, which correlateswith widespreaduse of antibiotics [1]. The sales of systemic anti-infective agents in general, particularly antibacterials and anti-tuberclotics, were greater in Iran than in three European countries. Broad-spectrum antibacterial agents accounted for a larger proportion of total sales in Iran [2]. The increase in pediatric allergy andasthma parallels the increase in the use of antibiotics. There isalso some evidence that antibiotic and/or paracetamol use mayincrease the risk of asthma. Antibiotics disturb the flora of the gastrointestinal tract, possibly perturbing the developing immune system[3]. Many lifestyle and medical care characteristics, including the use of antibiotics, have changed the patterns of infectious diseases and bacterial exposure in infancy in the past three decades. Antibiotic use, in addition to affecting the natural history of infection, is well-known to alter gut flora[3]. In industrializedcountries, the prevalence of asthma has increased significantlyover the last 30 years and is a major public health concern. Although the reasons for asthma epidemic are not clearlyunderstood, one hypothesis is that it is related to the exposureof infants to antibiotics. This is consistent withthe "hygiene hypothesis," which suggests that growing up ina more hygienic environment with less microbial exposure mayincrease atopic (T-helper type 2) immune responses, thus causingthe development of asthma. We studiedthe relationship between the use of oral antibiotics in thefirst year of life andasthma, allergic rhinitis, and eczema symptomsat the age 6-7 years in children. Subjects and Methods The study was fulfilled by analytic cross-sectional method in 6-7 year-old Yazdi students. Cluster sampling was applied and each school was used as a cluster. Sample size calculated by P=4% (prevalence of asthma), α= 0.05 and d=0.01 came to 1476 and regarding coefficient clustering and missing data, required sample size was set to 3000. The questionnaire was designed based on the questions from the International Study of Asthma and Allergies in Childhood (ISAAC); then the validity and reliability of the translated questionnaire were tested. Questionnaires were completed by parents who had children aged 6-7 years. The key asthma questions used were those on ‘wheeze ever’,‘wheeze in the last 12 months’, and ‘asthmaever’. The key rhinitis questionsused were those on ‘nose problems ever (sneezing or runny/blocked nose)’, ‘nose problems in the past 12months’, and ‘nose problems with itchy-watery eyesin the past 12 months’. The key eczema questions usedwere those on ‘eczema ever’, ‘itchy rash ever’(coming and going for 6 months), and ‘rash in the last12 months’. The data was first analyzed by Epi6 software and after being controlled, it was translated into SPSS 11.5 software. The results were then analyzed by using Chi-Square, Fisher-Exact, and ANOVA tests. Findings There was no significant relationship between early antibioticuse and ever wheezing (OR: 1.13, 95% CI: 0.77–1.67), wheezing during past 12 months (OR: 0.89, 95% CI: 0.41–1.95) and exercise-induced asthma (OR: 1.42, 95% CI: 0.82–2.47) but was associated with asthma ever (OR: 2.21, 95% CI: 1.05– 4.8). No significant relationship was found between the use of antibiotics with hay fever and eczema symptoms (Table 1). Antibiotic use during the first year of life was not significantly associated with 'ever hay fever' (OR: 1.22, 95% CI: 0.87–1.72) and eczema (OR: 1.3, 95% CI: 0.79–2.13) symptoms. Discussion In our previous study in Yazd city (central Iran) the prevalence of asthma, allergic rhinitis and eczema symptoms in children aged 6-7 years was 10.9%, 15.5% and 7.3% respectively[4].Also we showed the association of asthma with acetaminophen usage in the first year of life and indicated that using some drugs in infancy may be an important risk factor for the subsequent development of atopy and asthma [5]. Research on antibiotic exposure early in life and subsequentrisk of asthma and other allergic symptoms has yielded conflicting results. Many studies show that early antibiotic use is associated with the subsequent development ofwheezing and other allergic symptoms [3,6,7,8]. Wjstand colleagues examined a possible association of asthma epidemic and antibiotic use in a population-based study of 2,512 children aged 5-14 years in East Germany. They found that wheezing was associated with an increasing number of antibiotic courses (never versus one time OR 1.9, P= 0.012, 2 to 5 times OR 3.0, P<0.001 and more than 5 times OR 6.9, P<0.001) which was also seen for asthma diagnosis. The risk increased with earlier administration (never versus second year OR 4.6, month 7-12 OR 5.4 and birth until month 6 OR 7.9, all P<0.001)[9]. Kozyrskyj and colleagues found that independent from well-known asthma risk factors, asthmawas significantly more likely to develop in children who hadreceived antibiotics in the first year of life at age 7 years[10].The association with asthma was observed for antibiotic usein non-respiratory tract infections (adjusted OR1.86; 95% CI 1.02 to 3.37). The riskof asthma was highest in children receiving more than four coursesof antibiotics (adjusted OR, 1.46; 95% CI, 1.14 to 1.88), especiallyamong rural children, and in the absence of maternal asthmaor a dog in the birth year. Broad-spectrum (BS) cephalosporinuse was more common in these subpopulations of children[10]. Administration of broad-spectrum antibiotics, frequent practice inpediatric offices, impairs intestinal bacterial colonizationduring infancy [11]. Noverret al showed that antibiotic treatment in mice combined with fungalcolonization led to increased sensitization to anairway antigen and to pulmonary allergic responses[1]. In humans, the immune response of newborns is associated predominantlywith the helper T cell type 2 (Th2) cytokine phenotype, whereas rapid suppression of Th2 immune responses during thefirst year of life occurs in nonatopic children. Atopic individualsexhibit a continuation of fetal allergen-specific Th2 responsesduring infancy[12]. Because antibiotic use in infant mice leadsto alterations of the intestinal flora and impaired Th1 immuneresponses, it has been hypothesized that the previouslyobserved association between antibiotic use in early life andasthma in humans is due to antibiotic-induced changes in intestinalflora leading to a Th2-polarized immune deviation[13]. Nutten and colleagues found that antibiotic administration earlyin life negatively affects the specific immune response to aluminal antigen when it is first introduced during antibioticadministration. The increased mast cell numbers and mediatorconcentrations in the intestinal mucosa of the antibiotic-treatedanimals may testify the early stages of an altered immunesystem homeostasis[14]. On the other hand, many studies found no significant association between antibiotic use inthe first year of life and the subsequent risk of asthma, recurrent wheezing,allergic rhinitis, or eczema[15,16] . A US birth cohort study of high-risk children in the Boston area did not implicate antibiotic use in the first year of life as a risk factor for the outcomes of asthma and atopy at the age 5 years, as reported by parents[15].Foliaki and colleagues haveconducted an ecologic analysis of the relationship between antibioticssale and the prevalence of symptoms of asthma, allergic rhinoconjunctivitis,and atopic eczema in 99 centers from 28 countries. The result of this study showed a positive association betweenper capita antibiotics sale and the prevalence of symptomsfor asthma, rhinitis, and eczema, but the associations generallybecame negative once the analyses had been adjusted for Gross National Product (GNP). Their findings are generally not consistent withthe hypothesis that antibiotic use increases the risk of asthma,rhinitis, or eczema[17].Taken together, we found signi-ficant associationbetween treatment with oral antibiotics in the first yearof life and subsequent ever asthma (OR: 2.21, 95% CI: 1.05–4.80) but not with ever wheezing, wheezing during past 12 months and exercise-induced asthma at the age 6-7 years. Our study could be influenced by recall bias, as parentsof children with asthma may be more likely to report an exposureto antibiotics in infancy. Because of the limitationsof our study, additional prospectivestudies are needed to investigate the association between antibioticuse in early life and allergic symptoms in childhood. Conclusion Although there are sufficient reasons to avoid unnecessary use of antibiotics, particularly broad-spectrum agents, the results of our study do not support the association between antibioticuse in early life and allergic symptoms in childhood. Acknowledgment We are grateful to deputy for research in Yazd University of Medical Sciences and Health Services for financial supporting and all the mothers and children who took part in the study. Also thanks to Mr. Rokoee, Mrs Mobin, Mrs Rahim and thewhole ISAAC study team for their cooperation and help in data collection. Also thanks goes to MR Mozayan for his cooperation in editing the paper. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09022t1.jpg] |
| |||||||||

{kind=link}