 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
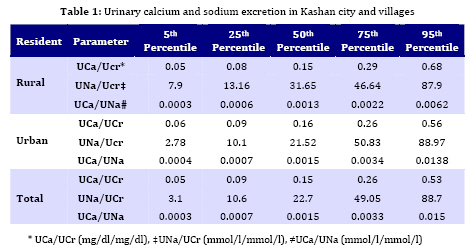
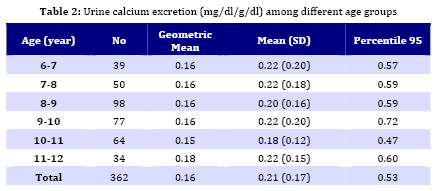
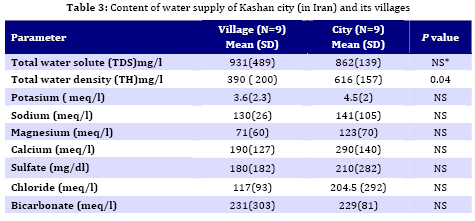
Iranian Journal of Pediatrics, Vol. 19, No. 2, June, 2009, pp. 154-158 Urinary Calcium Excretion in Healthy Children Living in Kashan/ Iran Ali Honarpisheh*1, MD;Nakysa Hooman2, MD; Abbas Taghavi1,MD 1. Department of Pediatrics, Kashan University of Medical Sciences, Kashan, IR Iran Received: Aug 20, 2008; Final Revision: Dec 05, 2008; Accepted: Feb 12, 2009 Code Number: pe09024 Abstract Objective:Urinary calcium excretion is different in various geographical regions. Therefore, we decided to evaluate the urinary calcium excretion in pediatric inhabitants of residential districts in the Desert of Iran and to determine the frequency of hypercalciuria. Key Words: Hypercalciuria; Urine sodium; Hematuria; School aged children; Urolithiasis Introduction Urinary calcium excretion might be influenced by genetic, age[1], geographic area, sun or light exposure[2,3], climate, drinking water[4] and nutrition[5]. Hyperacalciuria is defined as urinary calcium excretion more than 4 mg/kg/day which presents as abdominal pain, dysuria, frequency, hematuria, enuresis and urolithiasis, while most children with idiopathic hyprcalciuria are asymptomatic. Because of difficulty in collecting twenty four hour urine, a sample of urine is often used to calculate the urine calcium to creatinine ratio. If the ratio is higher than 0.21, it will be traditionally considered abnormal[6]. However; further investigations have shown that this cut point varies in different geographical areas[1,3,7,8]. In a cohort study Hingelfend et al[9] did not find seasonal variation of Uca/Ucr excretion in school aged children. Safarinejad[10] showed the mean ratio of 0.04 as reference value of urinary calcium excretion for all Iranian children; however, the sampling selection was not clarified. Another study from North of Iran near Caspian sea, reported the mean ratio of 0.15 among school children[11]. For this reason we decided to evaluate the urinary calcium excretion in pediatric inhabitants of Kashan, where water is supplied from Qanat. (Qanats are some hierarchial wells connected to each other that made manually and are specific for desert area in iran. These are made to reach the waterfills from the ground surface.) Subjects and Methods This is a descriptive study conducted in Kashan province from 2004 to 2005 which is one of the largest oases located at the margin of Central Desert (Dasht-e-Kavir) of Iran and has an estimated population of 272359 persons. Its water supply comes from a system of Qantas that cover up the oasis, the city also benefits from Solayman spring (a specific spring in desert of kashan city). By assuming 38.6%[4] as the prevalence of hypercalciuria, with 95% coefficient of confidence and 0.015 errors, the calculated sample size was 400 children aged 7-12 years. According to the last geographical map, 12 out of 53 villages were randomly selected. The city was divided into five districts: North, South, East, West and Center. By proportional cluster sampling 95 rural and 305 urban cases were selected. Every child was clinically examined and in case of having no sign of disease or history of excessive vitamin D intake, a questionnaire was completed. The urine sample was collected in a coded plastic sealed container and was sent to central laboratory of the University. Sodium, creatinine and calcium in urine samples were analyzed by RA1000 apparatus and flame-photometer. The mean, 25th, 50th, 75th, 90th and 95th percentiles were calculated. The children whose urine calcium to creatinine ratio was more than 0.2 were considered as hypercalciuric and those with urine sodium more than 200 meq/l hypernatriuric. Water samples were collected by health worker from 9 regions of the city and 9 villages for chemical analysis. The differences between frequencies were assessed by Chi square test; regression analysis was used to evaluate the correlation between variables. P values less than 0.05 were considered significant. Findings Thirty eight out of 400 randomly selected children refused to cooperate and were excluded from the study. Finally we evaluated 362 cases (139 males, 149 females), of which 288 were inhabitants of Kashan city and 74 (37 males, 37 females) were from outskirts (P>0.05). Mean age (SD) was 9.5 (1.47) and 9.47 (1.36) years in urban and rural groups respectively (P>0.5). Mean urine calcium to creatinine ratios were similar between the two groups (0.21±0.16). As shown in Table 1, the 95th percentile of urinary calcium, sodium excretion and urine calcium to sodium ratio were higher in rural children. Table 2 presents the urinary calcium excretion in different ages. As shown in Table 3, the contents of water were similar both in Kashan city and the villages, only mean total water density was higher in water supply of city (P<0.05). By regression analysis we found direct but weak correlation between urine calcium and urine sodium excretion (r=0.37, P=0.0001). Using traditional cut point of 0.21, the prevalence of hypercalciuria was 37.8 % from which 29.6% were urban and 8.3% rural inhabitants. On the whole, 5% of children (3.9% in city and 1.1% from villages) had 95th percentile value of Uca/Ucr that was greater than 0.53 mg/dl/mg/dl. Discussion This study showed that the overall urinary calcium excretion in school aged children at Kashan city and outskirts was higher than the previous report from Iran[10,11]. Safarinejad reported that 95th percentile of Uca/Ucr was 0.12 among children aged 7-12 years[10]. He found that sex, urine Na and K had no effect on this ratio. The same study in North of Iran[11] displayed that 95th percentile for urine calcium to creatinine ratio was three times higher than that of Safarinejad’s report. Our results points out that children living in desert have higher urinary calcium excretion compared to those who live near sea and in mountainous regions. This difference might be contributed to drinking water, habit of eating, or higher sun exposure. Urine sodium to creatinine ratio in our group was remarkablyhigher than in Safarinejad’s group. Unlike him we found a weak correlation between urine calcium and sodium excretion which is compatible with other studies. Another study from Thailand[12] showed a direct relation between urine calcium and sodium excretion. The 95th percentile value for Uca/Ucr in children living in desert area is significantly higher than reported values from Europe [13-16], Asia [3,12], America [7,8] and Turkey[18,17]. Five percent of children had 95th percentile value of Uca/Ucr; but using traditional cut point of 0.21, the prevalence of hypercalciuria was 37.8%. Geographical. genetic and environmental factors might be the reason for this wide discrepancy and it emphasizes more the finding of regional normal calcium excretion values. Drinking water of Kashan city and villages was analyzed and total water density was higher in city water supply. In a study performed by Kaneko et al[4] the prevalence of hypercalciuria was significantly higher in Aral Sea than the regions far from it and he meant tubular dysfunction be attributed to environmental chemical toxins or high sodium intake. One of limitations of present study was using the random urine calcium to creatinine ratio, which is a valuable screening test but the result needs to be confirmed by timed urine collection. In addition, the cases with hypercalciuria are prone to renal stone development; therefore, renal sonography should be recommended to those with hypercalciuria. Our study showed that urinary calcium excretion is high in desert of Kashan, thus it is important to conduct more studies to determine the risk factors and its untoward effects such as nephrolithiasis. Three recent published studies from Iran indicate that the cut point of UCa/UCr ratio more than 0.2 overestimates the diagnosis of hyprcal-ciuria[19-21]. Even though the urine calcium excretion was measured in healthy children, being aware of the impact of environmental factors on this ratio, we suggest that this ratio should be interpreted cautiously in diagnosing hypercalciuria and it should be confirmed by measuring calcium in a 24-hour urine aliquot. Conclusion This study showed that urinary calcium excretion is high in desert city of Kashan. Thus it is important to conduct more studies to confirm it by measuring calcium excretion in 24 hour urinary collection and to determine the risk factors and its untoward effects such as nephrolithiasis. It is important to establish a reference value for urinary calcium excretion in each geographic area. Acknowledgment This study was supported by Kashan University of Medical Sciences, grant No. 8222, dated 2004. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09024t2.jpg] [pe09024t3.jpg] [pe09024t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}