 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
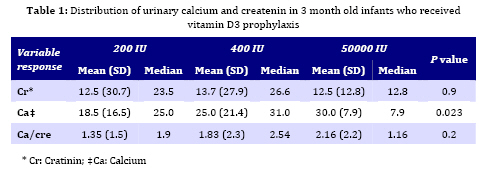
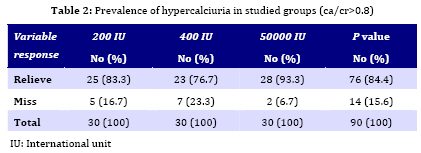
Iranian Journal of Pediatrics, Vol. 19, No. 2, June, 2009, pp. 159-162 Urinary Calcium/Creatinin Ratio with Different Dosages of Vitamin D3 Prophylaxis in Infants Ahmad Shajari1, MD; Mehrdad Shakiba1, MD; Forough Nourani1, MD; Maryam Zaki1, MD; Maryam Kheirandish1, MD 1. Department of Pediatrics, Shahid Sadoughi University of Medical Sciences, Yazd, IR Iran Received: Apr 16, 2008; Final Revision: Nov 24, 2008; Accepted: Jan 12, 2009 Code Number: pe09025 Abstract Objective: The requirement of vitamin D for breast-fed term infants remains an area of controversy. Different dosage is needed according to environmental factors such as sunlight exposure. Reception of more than 400 I.U. of vitamin D daily produces hypercalcemia. A random urine calcium/creatinin ratio (UCa/Cr) is a screening test for detection of hypercalciuria. Setting adequate values of vitamin D3 prophylaxis by random UCa/Cr in infant population of Yazd city in Iran, is the aim of present study. Key Words: Hypercalciuria; Vitamin D3-Prophylaxis; Calcium/Creatinin Ratio; Vitamin D; Infant Introduction Vitamin D is an essential element for establishing and maintaining bone structure. Vitamin D deficiency results in rickets and osteomalacia[1]. It is synthesized naturally in the skin after exposure to ultraviolet-B (UV-B) radiation from the sun. For any given infant or child, however, the amount of sunlight exposure (total surface area of the skin exposed for a given amount of time) needed to prevent vitamin D deficiency and rickets is difficult to determine; this is greatly influenced by the environment, including weather conditions, air pollution, time of year, and degree of latitude of the exposure[2]. The requirement of vitamin D for breast-fed term infants remains an area of controversy. The American Academy of Pediatrics Committee on Nutrition recommends Vitamin D supplementation for breast-fed infants only when the mother’s vitamin D nutrition has been inadequate, or if the infant does not benefit from adequate UV light exposure. Breast milk has vitamin D activity between 30–60 IU/L and would theoretically provide less than the recommended daily allowance for infants (400 IU/day). However, no evidence of vitamin D deficiency in unsupplemented healthy term breast-fed infants has been demonstrated[3]. For breast-fed infants residing above the 55thparallel or at lower latitudes with a high incidence of vitaminD deficiency, 800 IU/day (50000 IU/twice) are recommended during the winter months[4]. According to different environmental factors, reception of more than 400 IU of vitamin D daily produces hypercalcemia and its sequelae[5]. Hypercalciuria is implicated in the frequency-dysuria syndrome, abdominal pain, hematuria and urolithiasis, and defined as urinary calcium excretion of >4 mg/kg/day. Due to the difficulty of obtaining 24h urine collection in children, random urine calcium to creatinin ratio (UCa/Cr) is routinely used in clinical practice to screen for hypercalciuria, as it is found to have a good correlation with the 24h calcium excretion[6]. UCa/Cr of 0.21 has been regarded as abnormal and suggestive of hypercalciuria[7]. This study was done in a hot and dry area to measure urinary calcium/creatinin ratios with different dosages of vitamin D3 prophylaxis in breast fed infants. Subjects and Methods Case selection: Subjects were 90 fifteen day old healthy infants who had exclusively breast feeding. All of them weighed 2500-4100 gr. Exclusion criteria were having kidney disease, malnutrition and prematurity. Written informed consent was obtained from all parents. The research protocol was approved by the ethics committee on human experimentation of Yazd University of Medical Sciences. Subjects divided randomly into three groups and supplemented daily with 200 IU/daily vitamin D3 (Group I), 400 IU/daily vitamin D 3 (Group II) and the third group received 50000 IU vitamin D3 twice in fifteenth and sixtieth day after birth(Group III). Urine examination: Non-fasting urine specimen (between 9.30 am and 12.00 midday) was taken at the end of 3 months old. Urine calcium was measured by the cresolphthalein complexone spectro-photometric method and creatinine by Jaffle reaction. Both measurements were performed on COMAS-Mira automated analyzer (Roche Diagnostics, Mannheim, Germany). Serum 25-hydroxy-vitamin D was measured in all of infants. Statistical analysis:Mean urinary calcium and urinary creatinin was checked in each group and compared with Kruskal-Wallis test. Mean UCa/Cr in three groups analyzed with Kruskal-Wallis test. Mann-Whithney test in purpose of double cooperation of groups was done. Statistical analysis was performed on SPSS 7.5 andP<0.05 was considered significant. Findings Ninety healthy, term and breast fed infants enrolled in the study. Mean of urinary creatinin in Group I, II and III was 12.5, 13.7 and 12.5 respectively which was not significant (P=0.9) but mean of urinary calcium was 18.5, 25 and 30 respectively in three groups which was significant (P=0.02). It means that there is a relationship between hypercalciuria and different dosage of supplemented vitamin D. Mean of ca/cr ratio was 1.35, 1.83 and 2.16 in groups (Table 1). These differences were not significant (P=0.2). Prevalence of hypercalciuria was 83.3%, 76.7% and 93.3% respectively in three groups (Table 2). Comparison of mean value of ca/cr between groups by Mann-Whitney test showed that there was no significant difference between groups. Serum 25-hydroxy-vitamin D was normal in all infants (20 nanogram/mililiter). Discussion Vitamin D plays a critically important role in the development, growth, and mineralization of the skeleton during its formative years, and performs an equally essential role in maintaining a healthy mineralized skeleton for adults of all ages[8]. Enough usage of vitamin D is important for infants. Hypovitaminosis D is common in summer in exclusively breast-feeding infants[9] and clinical consequences of excessive vitamin D are secondary to hypercalcemia and Hypercalciuria[10]. It is important to remember that hypercalciuria usually precedes hypercalcemia as an indicator of vitamin D overdose[11]. In children, urinary ca/cr ratio is a useful and reliable method for determining hypercalciuria and also is a non-invasive and relative inexpensive method. In our survey, prevalence of hypercalciuria was 83.3% (group I), 76.7 % (Group II) and 93.3% (Group III) and total prevalence was 84.4%. More cases are needed to prove the relationship between hypercalciuria and different dosage of supplemented vitamin D. Although differences of ca/cr between groups were not significant but there was a numeral propensity (Table 1), so differences would be significant if the cases increased to 100 in each group. Hypercalciuria is likely present when a urinary random ca/cr ratio exceeding 0.21. Prevalence of hypercalciuria is different in different countries. The lowest prevalence is reported from Japan: 0.6%[12]. Reported prevalence in other countries has been 8.6%[13], 9.1%[14], 12-13% [15,16], 2.9% [17] in Germany,Italy,USA and Turkey respectively. In Tehran, Iran study on primary school children was 5.4%[20]. Differences may be related to different age groups. Hypercalciuria, the most common metabolic cause of pediatricurinary calculi, is not a single entity but rather a conditionassociated with many causes such as abnormal intake of vitamin D [21]. It was seen in this survey that hypercalciuria has direct relationship with vitamin D intake, so it is important to use proper amount of supplemented vitamin D. Conclusion It is recommended to use different dosages of prophylaxis in different regions. According to high prevalence of hypercalciuria in this survey, it is recommended to evaluate the vitamin D level in infants and use proper amount of supplemented vitamin D. It seems that 200 IU/daily could be used in infants in our area. Acknowledgment Authors thank all parents who helped us in managing the present study. The research protocol was approved by the research committee in Yazd University of Medical Sciences. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09025t2.jpg] [pe09025t1.jpg] |
| |||||||||

{kind=link}
{kind=link}