 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
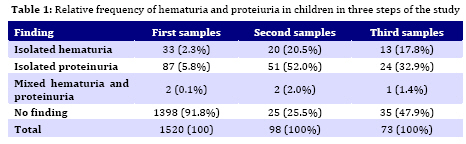
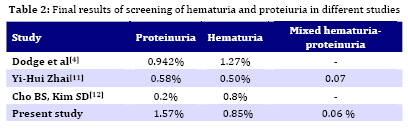
Iranian Journal of Pediatrics, Vol. 19, No. 2, June, 2009, pp. 169-172 Prevalence of Hematuria and Proteinuria in Healthy 4 to 6 Year Old Children in Daycare Centers of Rasht (Northern Iran) Hamidreza Badeli* 1, MD; Abtin Heidarzadeh2, MD; Mohammadreza Ahmadian3, MD 1. Department of Paediatrics, Guilan University of Medical Sciences, Rasht, IR Iran Received: Sep 03, 2008; Final Revision: Dec 01, 2008; Accepted: Jan 23, 2009 Code Number: pe09027 Abstract Objective: Screening of kidney diseases by urinalysis in preschool children was approved in many parts of the world with inexpensive tools such as urinary dipsticks. In this study the researchers investigate the prevalenceof hematuria and proteniuria in 4 to 6-year-old children in daycare centers of Rasht (Iran). Key Words: Proteinuria; Hematuria; Screening; Dipsticks; Urinalysis Introduction Screening of kidney diseases was of interest for the last three decades. For example, Japan[1] and USA[2] used urinalysis for screening in children and adolescents primarily with the commonly used dip-and-read test strips (dipsticks) mainly to detect proteins and hematuria. Hematuria and proteinuria are usually seen in primary period of systemic diseases and kidney diseases such as acute glomerulonephritis (acute post streptococcal glomerulonephritis), IgA nephropathy, membranoproliferative glomerulonephritis (MPGN)], nephrotic syndrome, hyper-calciuria, nephrolithiasis, renal tubular acidosis (RTA), congenital anomalies of kidney and urinary tract (CAKUT) such as polycystic kidney diseases, ureteropelvic junction stenosis (UPJS) and urinary tract infections (UTI)[3]. Early detection of these findings and diagnosis of the disease may facilitate preventing, halting and deferring the progression of some diseases. In unselected school-age children between 6 and 15 years of age, there was a prevalence rate of 3 to 4 percent of a positive dipstick for blood in a single urine sample [4,5]. This prevalence was decreased to 1 percent in two consecutive samples and 0.5 percent or less in three consecutive samples[6]. Demonstration of proteinuria in a routine screening urinalysis is common. As National Kidney Foundation Consensus Panel on Proteinuria, Albuminuria, Risk, Assessment, Detection, and Elimination (PARADE) reports, even after 4 tests, 10.7% of children have proteinuria in 1 out of 4 specimens [7]. In this study we screened 1520 children of Rasht day care centers for hematuria and Proteinuria. Subjects and Methods In this cross-sectional study children were sampled by multistage cluster sampling from day care centers of Rasht (Iran), the selected population consisted of 2390 children; 853 children did not deliver urine samples. 17 children were excluded due to the symptoms of urinary tract infections (fever, abdominal pain, vomiting, diarrhea, acute voiding symptoms), fever and history of kidney diseases. The first morning urine samples of 1537 remaining children were examined by urine strips (dipsticks) produced by Analyticone Co (Germany). An expert technician was employed to examine urine strips not later than an hour. Another urine sample of children with abnormal findings was examined with the same dipstick brand (used in the first analysis) a month later and if positive results were confirmed, a dipstick and microscope were used to examine a third urine sample. This study was approved by the ethics committees of Guilan University of Medical Sciences. Findings This study comprised 1520 children in the first dipstick urine analysis, out of which 870 were girls. In the first samples there were 122 abnormal samples (33 isolated hematuria, 87 isolated proteinuria and 2 mixed). For the second dipstick analysis 24 children did not submit their urine sample after a month. So in second stage of study, 98 cases delivered their urine samples. There were 73 abnormal urine samples (74.5%) in second stage. Finally, undertaken after a month, all 73 children delivered their urine samples. These were examined by dipsticks and microscopy. All data are shown for the whole three procedures in Table 1. The abnormal findings in all 1520 children were 13 (0.85%) isolated hematuria, 24 (1.6%) isolated proteinuria and one (0.06 %) mixed hematuria and Proteinuria in final samples (Table 2). Discussion Our study was designed to find out prevalence of hematuria and Proteinuria in children of day care centers in Rasht (Iran) in comparison to other similar studies. Although we analyzed urine just with dipstick in first samples, and near 20% of children did not deliver urine for the second analysis, the third samples of the survey revealed that 13 (0.85%) isolated hematuria, 24 (1.57%) isolated proteinuria and one (0.06%) mixed hematuria and Proteinuria existed in the tested pediatric population. National Japanese Urinary Screening Program which was conducted to evaluate elementary school children and junior adolescents revealed that there was 1.88% hematuria in elementary school students and 5.13% in the first screening urine samples of adolescents which fell to 0.54% and 0.94%, respectively, on the repeated screening urinalyses[1]. Among the school children identified with persistent isolated hematuria in these studies, 18% had a diagnosis after their comprehensive evaluations were completed[7]. Dodge et al conducted three consecutive urinalyses on 6 to 12 year old children at intervals of 3-6 weeks and found proteinuria in all three tests in 0.942% of females, 0.33% of males, and hematuria in 0.34% and 0.12%, in that order[8]. Although Kaplan and colleagues stated that multiple screening dipstick urinalyses in asymptomatic pediatric patients are costly and should be discontinued but they proposed a single screening dipstick urinalysisbe obtained at school entry age, between 5 and 6 years, inall asymptomatic children[3]. The study of Yong-Hoon Parkand colleagues showed that the use of a mass school urine screening program may detect chronic renal disease in its early stage and recommend that more attention should be paid to identify those children with combined proteinuria and hematuria and massive proteinuria[9]. Kawasaki et al found that early identification by yearly school urinary screening may enableearly management and improve prognosis for MPGN type 1 in children [10]. Although our study had a different prevalence rate, alike other above mentionedarticles it found abnormalities that can be meaningful for indicating its impact. Screeningtests such as hearing and visual assessment, blood pressure, growth and development, behavioral disturbance, dental and general physical examination are being conducted in all preschool children in Iran. If dipstick urinalysis with its inexpensive costs could be added to our country’s screening program for this period of life, it could contribute to detection of the affected children in early stages of renal diseases, resulting in the survival of’ kidneys at risk. Conclusion This article determined the prevalence of proteinuria and hematuria in preschool children in Rasht day care centers which showed findings rather similar to other related studies. It was also found that it would be possible to screen a large population of children at a relatively low cost, providing the frame work for further action that may lead to the prevention and timely diagnosis of renal diseases. Acknowledgment The authors thank Dr B Sardar Noori and his colleagues for their help and advices in preparing laboratory data. We would also like to thank Mr E Ezati for his valuable comments. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09027t1.jpg] [pe09027t2.jpg] |
| |||||||||

{kind=link}
{kind=link}