 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
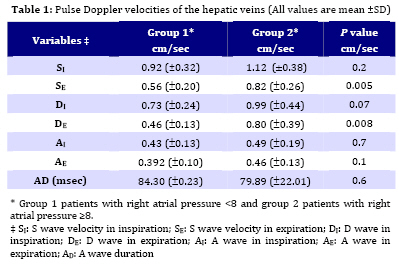
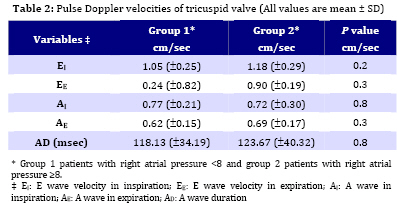
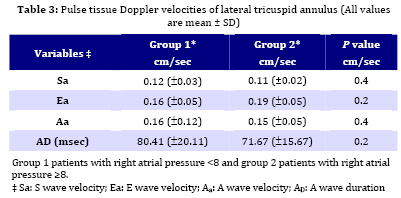
Iranian Journal of Pediatrics, Vol. 19, No. 3, Sept, 2009, pp. 224-230 Relation of Mean Right Atrial Pressure to Doppler Parameters of Right Atrial and Hepatic Venous Flow in Pediatric Patients with Congenital Heart Disease Hamid Amoozgar1, MD; Khobiar Zare1, MD; Mohammad Borzoee1,MD; Gholamhossein Ajami1, MD; Saeid Abtahi1, MD 1. Division of Pediatric Cardiology, Shiraz University of Medical Sciences, Shiraz, IR Iran Received: Nov 11, 2008; Final Revision: Mar 17, 2009; Accepted: Apr 11, 2009 Code Number: pe09034 Abstract Objective:A paucity of data exists regarding the relation of mean right atrial pressure (RAP) to Doppler parameters of right atrial and ventricular filling in pediatric patients with congenital heart disease. Key Words: Diastole; Echocardiography; Ventricles; Pressure; Atrium Introduction The estimation of right ventricular filling pressureis important clinically for the diagnosis and management ofvarious hemodynamic conditions [1-4]. Furthermore, assessmentof right atrial pressure (RAP) is needed in the echocardiographylaboratory for estimation of systolic right ventricular, pulmonary artery pressures and left atrial pressure [5-8]. Although clinical evaluationof jugular venous pulsations is usually used to estimate RAP,it may be difficult in children with short neck, and such an examination may not always be feasiblein a busy echocardiography laboratory [6,7]. A few studies in selectedadult patients have evaluated the right-side hemodynamic correlatesof right atrial and right ventricular filling dynamics[9,10,11]. Tricuspid and hepatic venous flow dynamics have been describedin patients with restrictive cardiomyopathy[10] and have beenused to help differentiate constrictive pericarditis from restrictive cardiomyopathy[11,12]. On the other hand, studies on the changes in the diameterof the inferior vena cava in response to negative intrathoracic pressurehave demonstrated a significant relation of this index to RAP [13-19]. Such an approach, however, requires the patient'scooperation and has been limited in mechanically ventilated individuals[15]. A comprehensive evaluation of the relation of echocardiographicand Doppler parameters of right ventricular function, right atrialfunction, and inferior vena cava to mean RAP in pediatric patients witha variety of clinical conditions has not been performed previously. Because several of these parameters can be obtained from routinecardiac ultrasound examination, it is important to evaluatewhich of these parameters has the best correlation with RAP and whethera combination of these indexes improve the clinical estimationof right ventricular filling pressure. Accordingly, this studywas undertaken to assess the relation of Doppler parametersof hepatic vein, tricuspid inflow and pulse tissue Doppler imaging (TDI) of lateral tricuspid annulus. Subjects and Methods Fifty pediatric patients with congenital heart disease who needed right sided interventional or diagnostic cardiac catheterization were enrolled in this study consequently from April 2007 till June 2008. Echocardiography was performed with a GE vivid 3, 3 MHz probe and TDI software. Hepatic veins systolic (S), diastolic (D), atrial reversal flow (A) and its duration were recorded in inspiration and expiration. Tricuspid early diastolic (E) and late diastolic (A) were also recorded in apical four chamber view in inspiration and expiration. Tissue Doppler imaging was obtained with the sample volume placed at the lateral corner of lateral tricuspid annulus from the apical four chamber view. In each region, systolic (S) wave, early diastolic (Ea), and late diastolic (Aa) velocities were also recorded. Echocardiographic data gathered from echocardiography of each patient was then compared with the result of cardiac catheterization. The investigational protocol was approved by the research committee at the Shiraz University of Medical Sciences, and written informed consents were obtained from each patient or parents.All data are expressed as means ± one standard deviation (SD), linear regression was used to examine the relationship between echocardiographic parameters and angiographic mean right atrial pressure. Non parametric tests used for analysis between two independent samples. Pearson product moment correlation was used to compare values obtained by the two methods. Linear correlation was also tested using the Spearman rank method (correlation coefficient with 95% confidence interval). A receiver operating characteristic (ROC) curve was generated for statistically significant echocardiographic parameters, varying the discriminating thresholds of these parameters to determine the ability of mean right atrial pressure to discriminate between patients with a high right atrial pressure and those without it. MedCalc® 8.0 software was used for statistical analysis. Findings From fifty pediatric patients who enrolled in this study 30 patients were male and 20 female. Mean (±SD) age of patients was 4.96 (±4.05), mean body surface area 0.56 (±0.25). The diagnoses consisted of tetralogy of Fallot (23), ventricular septal defect (10), pulmonary stenosis (3), atrial septal defect and pulmonary stenosis (2), primary pulmonary hypertension (4), dilated cardiomyopathy (1), ventricular and atrial septal defect (2), coronary fistula (1), patent ductus arteriosus (1), patent ductus arteriosus and coarctation of aorta (1), transposition of great artery and pulmonary stenosis (2). Patients were categorized in two groups according to their RAP that was measured by cardiac catheterization: Group 1 (40 patients) consisted of cases with mean RAP <8 mmHg and group 2 (10 patients) of those who had mean RAP ³8mmHg. Pulse Doppler echocardiographic data of hepatic vein, tricuspid annulus and TDI of lateral tricuspid annulus are recorded in Tables 1, 2 and 3. Due to statistically significant correlation of peak E to A velocity ratio of tricuspid valve in expiration, peak S to D velocity ratio of hepatic vein in expiration and change in a velocity of tricuspid valve in respiratory cycle, linear regression equation was used as follows: 1) RAP= [A tricuspid change ´ (-0.01)]+ 6.5 (P<0.001, r=0.38) A: velocity of atrial contraction wave 2) RAP= [S/D (IVC flow in expiration)´0.96]+ 5.01(P<0.001, r=0.43) S: velocity of systolic wave of IVC flow D: velocity of diastolic wave of IVC flow 3) RAP= [E/A (tricuspid flow in inspiration)´1] + 4.85 (P<0.001, r=0.37) E: velocity of early diastolic wave of tricuspid A: velocity of atrial contraction wave of tricuspid flow ROC curves showed that if S wave velocity change of hepatic vein in respiration was more than 38%, sensitivity and specificity of having a RAP more than 8 mmHg was 90% and 51.3% respectively with positive likelihood ratio (+LR) of 1.85 and negative likelihood ratio (-LR) of 0.19; A peak S wave velocity of less than 70 mm/sec also shows a RAP more than 8 mmHg with sensitivity and specificity of 70 and 82.1 respectively (+LR=3.9, -LR=0.37). An expiratory peak D wave velocity of hepatic vein more than 63 mm/sec is indicator of RAP more than 8 mmHg with sensitivity and specificity of 60% and 92.3% respectively (+LR=7.8, -LR=0.43). An inspiratory E to A velocity of tricuspid wave more than 1.88 is indicator of RAP more than 8 mmHg with sensitivity and specificity of 60% and 82.5% respectively (+LR=3.43, -LR=0.48), and inspiratory Ea to E velocity ratio more than 11.8 is indicator of RAP more than 8 mmHg with sensitivity and specificity of 60% and 87.5% respectively (+LR=4.8, -LR=0.46). Discussion Estimation of RAP is helpful in the overall management of patients withhemodynamic disorders and in the derivation of pulmonary arterypressure or left atrial pressure with Doppler echocardiography [20]. The phases of hepatic venous flow in normal individuals were described[15]. Determinants of the systolic forward flow includeatrial relaxation, descent of the tricuspid annular plane towardthe ventricular apex, and RAP[21,22,23]. In higher RAP, the pressure gradient between the hepatic veins and the rightatrium will be lower and thus the forward systolic flow will be lower. This observationwas described previously in patients with restrictive heartdisease and elevated filling pressures[24,25]. In the presentstudy, decrease in systolic (S) forward flow parameters and increase in diastolic venous flow (D) had fine relation to mean RAP and allowed a goodestimation of atrial pressure in patients with a variety of underlyingclinical conditions. With respiratory variability present in any right-side Dopplervelocity recording, measurements were performed as an averageof several consecutive beats, which yields results similar tothose obtained during end-expiratory apnea[16]. This allowedassessment of RAP in patients with dyspnea or on mechanical ventilationin whom the relation of systolic filling fraction with RAP provedto be similar to those without assisted ventilation. Exclusionsrelated mostly to nonsinus rhythms and occasional technical difficultiesin patients in the Intensive Care Unit. Unlike recordings ofpulmonary vein flow[26]. Doppler assessment of hepatic vein flowwith transthoracic approach is simpler and feasible in the majorityof patients even in Intensive Care Units, as shown in this study,thus allowing assessment of RAP in most patients. The present study showed good correlation between cyclic respiratory changes in peak S wave velocity and mean RA pressure. Although there were statistically significant correlations between Peak E to A velocity of tricuspid valve in expiration, peak S to D velocity of hepatic vein in expiration and change in A velocity of tricuspid valve in respiratory cycle, linear regression equation showed not a strong estimation of mean RA pressure by this model. This data is against the studies in adult patients without structural heart disease[18]. Among all parameters tested,hepatic vein systolic wave velocity, diastolic wave velocity and changes of S wave velocity phasic changes during respiratory cycle have provided useful yet simple indexes for the assessmentof mean RAP in pediatric patients with CHD. Determination of these parameters provideda reasonable estimate of high mean RAP. Doppler recordings of tricuspid inflow, however,are also important in the overall evaluation of right-sided hemodynamicsand hepatic venous flow. Assessment of these parameters corroboratesfindings of atrial filling dynamics and is important when derivationof mean RAP cannot be performed noninvasively. Conclusion This study showed that hepatic venous flow can be valuable for estimation of mean RAP in pediatric patients with congenital heart disease. It is noteworthy to mention the characteristics of patientsin whom the observed relations in this study may not be applicable;these include patients with non-sinus rhythm, pericardial diseases and also patients with severe tricuspidregurgitation, who usually have reversal of systolic hepaticvenous flow, were not included in this study. Acknowledgment The authors thank the Office of Vice Chancellor for Research of Shiraz University of Medical Sciences for financial support of this study. They also thank Professor Gholamhossein Amirhakimi for thoughtful reviewing of the manuscript. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09034t1.jpg] [pe09034t3.jpg] [pe09034t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}