 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
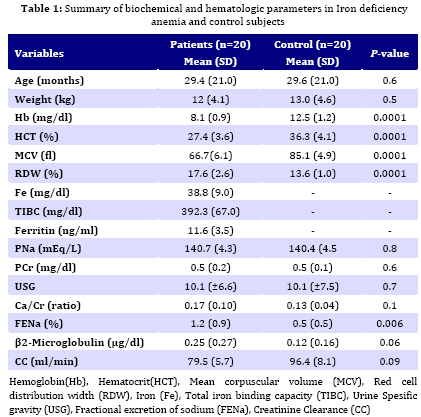
Iranian Journal of Pediatrics, Vol. 19, No. 3, Sept, 2009, pp. 231-236 Renal Tubular and Glomerular Function in Children with Iron Deficiency Anemia Simin Sadeghi-Bojd1,2, MD;Mohammad Hashemi3,4*, PhD; Forood Salehi1, MD 1. Department of Pediatrics, Zahedan University of Medical sciences, Zahedan, IR Iran Received: Oct 01, 2008; Final Revision: Feb 06, 2009; Accepted: Mar 19, 2009 Code Number: pe09035 Abstract Objective:Iron deficiency anemia (IDA) resulting from lack of sufficient iron for synthesis of hemoglobin is most common hematologic disease of infancy and childhood. There is little information about the renal function in iron deficiency anemia. The aim of the present study was to examine the renal function in children with iron deficiency anemia. Key Words: Iron deficiency; Anemia; Renal tubular function; Glomerular function Introduction Iron deficiency anemia (IDA) is the most common nutritional deficiency in children. The World Health Organization estimates that anemia, largely caused by iron deficiency affects between 500 million and two billion people worldwide. The prevalence of IDA is high in children of undeveloped countries [1]. It has a negative influence on growth and mental status [2]. Iron (Fe) is an essential nutrient in humans. The majority of iron (75 percent) is bound in heme proteins such as hemoglobin and myoglobin. The remainder is bound in the storage proteins ferritin and hemosiderin with a small portion (3 percent) bound in critical enzyme systems, such as catalase and cytochromes [3]. In normal subjects, only a small amount of iron enters and leaves the body on a daily basis. Most iron is recycled from the breakdown of old red blood cells by macrophages of the reticuloendothelial system. About 30-50 percent of women and children have IDA in Iran [4]. Kadivar et al[5] reported that the prevalence of IDA was 19.7% in 6 month to 5 year old children in Fars, Southern Iran. In southwest Iran 43.9% of the children are anemic, and 29.1% have iron-deficiency anemia [6]. Iron deficiency has deleterious effects on cell respiration, mitochondrial oxidative properties, and the electron transport chain, [7]. There is little information about the renal function in IDA. Ozcay et al reported that children with iron deficiency anemia had impaired renal tubular function[7]. The purpose of this study was to evaluate renal function in children with IDA. Subjects and Methods This case-control study was performed on 20 pediatric patients with IDA (mean age 29.54 months, range 6-72 months) and 20 healthy children (mean age 29.6, range 6-72 months) served as controls. The subjects were selected via convenience sampling. This study was approved by ethics committee of Zahedan University of Medical Sciences and informed consent was obtained from parents of the subjects. Subjects with urinary tract infection, malnutrition, renal disease, G6PD deficiency and hemoglobinopathy were excluded. Blood sample was obtained to determine hemoglobin (Hb), hematocrit (HCT), mean corpuscular volume (MCV) and red blood cell distribution width (RDW) from each subject. Control group consisted of children with normal Hb, HCT, MCV, RDW. If Hb, HCT, MCV and RDW suggested IDA (Hb<10.5 gr/dl, HCT<32 %, MCV<72 fl, RDW>15 %), serum iron level, iron-binding capacity and ferritin were determined. Percent of transferrin saturation was calculated from: (% transferring saturation=(Fe/TIBC)×100 Serum iron level <50 mg/dl, iron binding capacity >350 mg/dl, ferritin level <12 ng/ml and transferrin saturating <15% suggested iron deficiency anemia [7]. We also obtained 24 hr urine from case and control using catheter and creatinine clearance (CC) which is a good approximation of glomerular filteration rate. GFR was calculated from the formula; GFR ≈ (urine creatinine concentration×urine volume)/ plasma creatinine concentration Urine tested for specific gravity. The levels of β2-microglobulin, creatinine, sodium, and calcium were measured using commercially available kits. Statistical analysis was performed using SPSS (version 11). Data were expressed as mean (±SD) and compared between two groups by unpaired t-test. A two-tailed P value less than 0.05 was considered statistically significant. Correlations were analyzed with Pearson’s correlation coefficient test and P value less than 0.05 was considered statistically significant. Findings The demographic parameters, hematological and biochemical parameters of IDA patients and healthy subjects are shown in Table 1. The levels of Hb, HCT, MCV, RDW had statistically significant difference between case and control (P=0.0001). In IDA group, the levels of iron, total iron binding capacity (TIBC) and ferritin were 38.8 (±9.0) mg/dl, 392.3 (±67.0) mg/dl and 11.6 (±3.5) ng/ml, respectively. As shown in Table 1, the serum levels of sodium and creatinine were not significantly different between IDA and control group (P>0.05). Fractional excretion of sodium (FENa) was significantly higher (P=0.006) in IDA group than in control group. The level of β2-microglobulin in urine was higher in IDA patients than in control group, but the difference was not statistically significant. Also, urine specific gravity and calcium/ creatinine (Ca/Cr) ratio were not significantly different between case and control group. The result showed that the creatinine clearance was not significantly different between IDA and control group, although the level of CC in patients was lower than in control group. There was no correlation between FENa and Hb (r=0.13, P=0.6), FENa+ and Fe+2 (r=0.08, P=0.7), FENa+ and TIBC (r=-0.08, P=0.7), FENa+ and ferritin (r=0.04, P=0.9) as well as Hb and β2-microglobulin (r=0.02, P=0.4) in IDA patients. Discussion Anemia resulting from lack of sufficient iron for synthesis of hemoglobin is the most common hematologic disease of infancy and childhood. Its frequency is related to certain basis aspects of iron metabolism and nutrition. Iron deficiency has serious effects on cardiovascular and nervous system but there are not enough studies about effect of IDA on renal function. We found that there were no significant differences between IDA and control group regarding serum sodium and creatinine, urine specific gravity, urine β2-microglobulin, Ca/Cr ratio and creatinine clearance (CC). We observed that FENa was significantly higher in IDA patients than in control group. The level of urine β2-microglobulin was higher in IDA patients than in controls although it was not statistically significant. We also found that the level of CC was lower in patients than in control group without statistically significant difference. Ozcay et al [7] reported that FENa and urinary N-acetyl-β-D-glucosaminidase/ crea-tinine were significantly higher in the children with iron deficiency anemia than in control group while they found no differences between IDA and control groups regarding serum sodium and creatinine, urine osmolality, urine microalbumin level, and Ca/Cr ratio. Our results are in agreement with this study. FENa reflects mainly proximal tubular damage as proximal tubule reabsorbs sodium three times as much as the distal tubule does[8]. We found no correlation between FENa and Hb, FENa+ and Fe+2, FENa+ and TIBC, FENa+ and ferritin as well as Hb and β2-microglobulin in IDA patients. Ozcay et al [7] had found no correlation between FENa and hemoglobin level and the result is in agreement with our finding. Kaissling et al [9] demonstrated that the most striking anemia related morphological change was damage to the proximal tubule. In tissues from anemic rats, the authors observed focal proximal tubular necrosis in the renal cortex but no structural signs of hypoxia in the medulla. Mehta et al [10] found that three hour creatinine clearance was impaired in IDA, and it improved after 3 days of intravenous iron therapy. Since no significant hemoglobin rise was observed with iron administration, they concluded that iron effect at the tissue level is independent of the anemia. Increased urine β2-microglobulin is a reliable indicator of proximal tubular damage. Urinary excretion of β2-microglobulin is increased in a variety of diseases that impair proximal tubule such as iron toxicity, and minor or major thalassemia [11-13]. In this study urine β2-microglobulin was higher in IDA patients than in controls although statistically not significant. There was no correlation between Hb level and urine β2-microglobulin level. Ozcay reported that Hb level was negatively correlated with urineN-acetyle-β-D-glucosaminidase /Creatinine (NAG/Cr) and patients with IDA had a higher NAG/Cr than control group which indicates proximal tubular damage in the anemic group[7]. Thalassemia patients have a high prevalence of renal tubular abnormalities.Renal dysfunction in thalassemia patients can be attributed to chronic anemia and iron overload as well as to desferioxamine toxicity [12,13]. The severity correlated with the degree of anemia, being least severe in patients on hypertransfusion and iron chelation therapy, suggests that the damage might be caused by anemia and increased oxidation induced by excess iron deposits [11]. Cetin et al [14] reported that 14.6% of patients with β-thalassemia minor showed significant signs of renal tubulopathy. In a study on women in general population in Japan no tubular dysfunction was observed among women with iron deficiency [15]. Previously we studied renal tubular function in patients with β-thalassemia major. The results showed significant signs of renal tubulopathy, such as hypercalciuria (12.9%), proteinuria (8.6%), phosphaturia (9.2%), magnesiumuria (8.6%), hyperuricos-uria (38%) and excretion of β2 microglobin (13.5%) [16]. Alaei et al [17] in a descriptive study investigated probable defects in tubular reabsorption of sodium, potassium, phosphate and protein in children with IDA. They found that 87% of patients had at least one indicator of tubular dysfunction and concluded that the prevalence of tubular dysfunction was high in IDA children. The investigators had no control group and the parameters were determined on random urine samples. Although iron deficiency anemia is common, we investigated the study in 20 IDA and 20 healthy subjects due to weak cooperation of parents, especially in infants. Conclusion In this study we investigated renal tubular and glumerular function in children with iron deficiency anemia. We found that in IDA the level of β2-microglobin was higher than in normal individuals although it was not statistically significant. In addition, FENa was significantly higher in IDA than in normal subjects. The findings showed evidence of tubular damage in IDA which needs further investigation. Acknowledgment This work was supported by a research grant from Zahedan University of Medical Sciences, Zahedan, Iran. The authors would like to thank the patients and healthy subjects who willingly participated in the study. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09035t1.jpg] |
| |||||||||

{kind=link}