 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
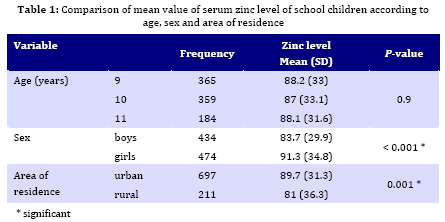
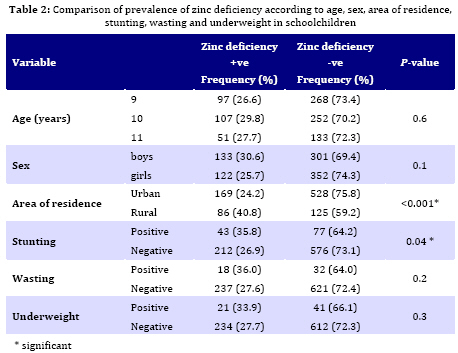
Iranian Journal of Pediatrics, Vol. 19, No. 3, Sept, 2009, pp. 249-254 Prevalence of Zinc Deficiency in Elementary School Children of South Khorasan Province (East Iran) Azita Fesharakinia* 1, MD; Asghar Zarban2, PhD; Gholam-Reza Sharifzadeh3, MSc 1. Department of Pediatrics, Birjand University of Medical Sciences, Birjand, IR Iran Received: Sep 26, 2008; Final Revision: Feb 06, 2009; Accepted: Feb 25, 2009 Code Number: pe09038 Abstract Objective: Zinc deficiency is common in developing countries and can affect growth of children. The objective of this study was todeterminethe prevalence of zinc deficiency and its effect on growth in elementary school children of South Khorasan province. Key Words: Zinc deficiency; Elementary school children; Prevalence; Growth; Iran Introduction Zinc has been shown to be an integral constituent and cofactor of more than 100 metalloenzymes that play an important role in DNA, RNA and protein synthesis[1]. World wide zinc deficiency could rival the documented iron deficiency[2]. Zinc deficiency is one of the ten biggest factors contributing to burden of disease in developing countries with high mortality[3]. The prevalence of a moderate zinc deficiency of 5-30% has been reported in children and adolescents of different countries[4]. Zinc is an essential trace element involved in normal growth and development[5]. Zinc deficiency affects the growth hormone metabolism, and may be a limiting factor in growth regulation [6,7]. Zinc deficiency is associated with poor growth, depressed immune function, hair loss, increased susceptibility to and severity of infections and neurobehavioral abnormalities [8-11]. In many lower-income countries, zinc deficiency is common because the diets are composed primarily of cereals and legumes, whichcontain substantial amounts of phytate a compound known to inhibit zinc absorption and few animal-source foods (muscle meats or organs), which arerich sources of zinc and are free of phytate [2]. Moreover,approximately one-third of children in low-income countrieshave a low height-for-age relative to international referencedata. Thus, zinc deficiencyappears to be widespread in lower-income countries, and interventionprograms are needed to improve zinc status in these high-riskpopulations. Experiences from animal and human studies indicate that retarded growth velocity is an early and potentially reversible manifestation of even mild zinc deficiency [12]. In a wide study by Sharify et al [13] in 1996 on 1180 school children aged 8-11 years in 23 provinces of Iran (was not studied in Khorasan province), 13.7% of students were zinc deficient and in a study in Birjand (the center of South Khorasan province: east of Iran) the prevalence of growth retardation was high in elementary school children [14]. So this study was performed for the first time in this province in order to determine the prevalence of zinc deficiency and its relation with growth retardation in elementary school children. Subjects and Methods This cross-sectional study was carried out on 908 school children aged 9-11 years in South Khorasan province from October to December 2007. The ethics committee of the Birjand University of Medical Sciences approved the study. Schools were stratified according to location (urban, rural). From each stratum, a proportional, two stage cluster sample of children was selected. The primary units (clusters) were the schools (31 schools). The secondary were the students within the schools and equal numbers of children were sampled from each school. Children were allocated with code numbers and randomly selected using random number tables. A questionnaire included age, sex and residence area of each individual that was completed by one of parents. Weight was measured to the nearest 0.1 kg (Seca Beam Balance) with the subjects lightly dressed and bare foot. Standing height to the nearest 0.1 cm (Seca Stadiometer) was also recorded. The SD scored for height-for-age (HAZ), weight -for-age (WAZ) and weight-for-height (WHZ) were calculated in comparison to the National Center for Health Statistics (NCHS) standard population. Stunting, underweight and wasting were defined as HAZ≤-2, WAZ≤-2 and WHZ≤-2, respectively [15]. Blood samples were collected in the morning from fasting subjects for zinc analysis. The blood was centrifuged at 2500 rpm at 4°C for 10 min to obtain the serum. The serum was stored at -20°C until analyzed. Serum Zinc level was estimated by Shimadzu 6300 atomic absorption spectrophotometry. The analytical wavelengths were set at 214.0 nm. All serum samples were diluted (1:5) with deionized water. Standard solutions of Zinc were prepared by dilution of certified standard solutions. Dilute working standard solutions were prepared immediately prior to their use by stepwise dilution of the stock standard solution with 5% glycerol to obtain same viscosity of the serum samples. All glassware used for the zinc analysis had been previously soaked in diluted nitric acid (10%) for 2 hours and thoroughly rinsed with deionized water to avoid any zinc contamination. Results were documented in terms of μg/dl. Zinc deficiency was defined as serum zinc < 70 μg/dl [16]. Statistical analysis was performed by the SPSS statistical package using t-test, Chi-square and ANOVA. A P-value less than 0.05 was considered to be significant. Findings This study was carried out on 908 school children aged 9-11 years. 474 subjects (52.2%) were girls. 697 subjects (76.8%) resided in city. The prevalence of stunting, underweight and wasting was 13.2%, 6.8% and 5.5%, respectively. The mean value of zinc level was 87.7 (±32.7) μg/dl and it was significantly higher in girls and urban areas (Table 1). There were no significant differences in mean serum zinc level in school children with normal growth and subjects that were stunted, underweight or wasted. 255 (28.1%) school children were zinc deficient. The prevalence of zinc deficiency was significantly higher in rural area than in urban area and it was not related significantly with age and sex of school children (Table 2). The prevalence of zinc deficiency was significantly higher in stunted school children than non-stunted school children (Table 2). Discussion In present study the mean zinc level was 87.7 (±32.7) μg/dl and it was significantly higher in girls and in urban areas with no difference in age. In Sharifi study [13], the mean zinc level was 115 ±42 μg/dl and it was not significantly different according to sex and area of residence. In another study in Tehran[17] on 881 students with the mean age of 13.2 ±1.0 yr, the mean (SD) was 95.2 (±17.7) μg/dl. In a study in Venezuela [18] in 320 children aged 7-14 years, there was a tendency for serum Zinc to increase with age and there was no significant difference in zinc levels according to sex. In a study in Greece [19] in 105 children aged 3-14 years, the mean level of zinc was 97.5 μg/dl (15 μmol/l) with no significant difference between boys and girls; a significant positive correlation was found between Zinc levels with age and height-for-age. In a study on 156 Japanese children (6-12 years old) the average serum zinc concentration was 92 (±13) μg/dl with no significant differences according to sex and age [20]. In a study in 58 children (3 months-5 years) in India [21], there was a significant positive correlation between serum zinc and height-for-age. In present study 28.1% of children were zinc deficient. The prevalence of zinc deficiency was significantly higher in rural areas with no difference according to sex and age. In Sharify study[13] 13.7% of subjects were zinc deficient (13% boys and 14% girls) and the prevalence of zinc deficiency was different in different provinces. In Tehran study[17] the prevalence of zinc deficiency was 31.1% and its prevalence was significantly higher in male children.In a study in Sri Lanka on 945 school children of the age group 12-16 years zinc deficiency was found in 51.5% and 58.3% of boys and girls, respectively [22]. In present study the prevalence of zinc deficiency was significantly higher in stunted school children than non-stunted school children. Some studies [23,24,25] showed that in children with short stature, zinc supplementation increases growth velocity. A study in Iran [26] showed that after 7 months zinc supplementation in 804 school children aged 8-12 years, significant increase in weight and length growth was found. Another study in Iran showed that zinc supplementation of malnourished school boys significantly increased height, weight and bone age [27]. Present study has a few limitations. The dietary intake and the mean intake of zinc were not assessed and in stunted children the effects of zinc supplementation on length growth must be assessed. Conclusion The present study showed that zinc deficiency is common in school children of South Khorasan province and is related significantly with stunting, so searching studies for underlying factors of zinc deficiency, dietary assessment of zinc intake and zinc supplementation especially in stunted children is recommended. Acknowledgment This study was supported by a grant from Research Center of Birjand University of Medical Sciences. We would like to express our thanks to the children who participated in this study. References
© 2009 by Center of Excellence for Pediatrics, Children’s Medical Center, Tehran University of Medical Sciences, All rights reserved. The following images related to this document are available:Photo images[pe09038t2.jpg] [pe09038t1.jpg] |
| |||||||||

{kind=link}
{kind=link}