 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
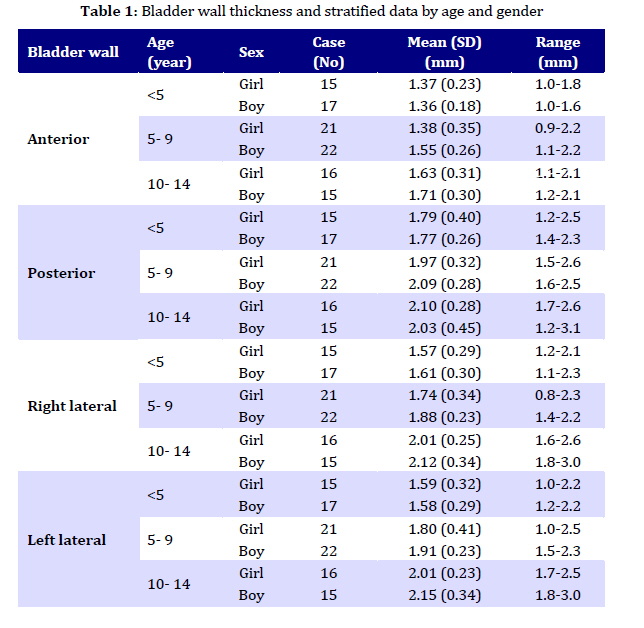
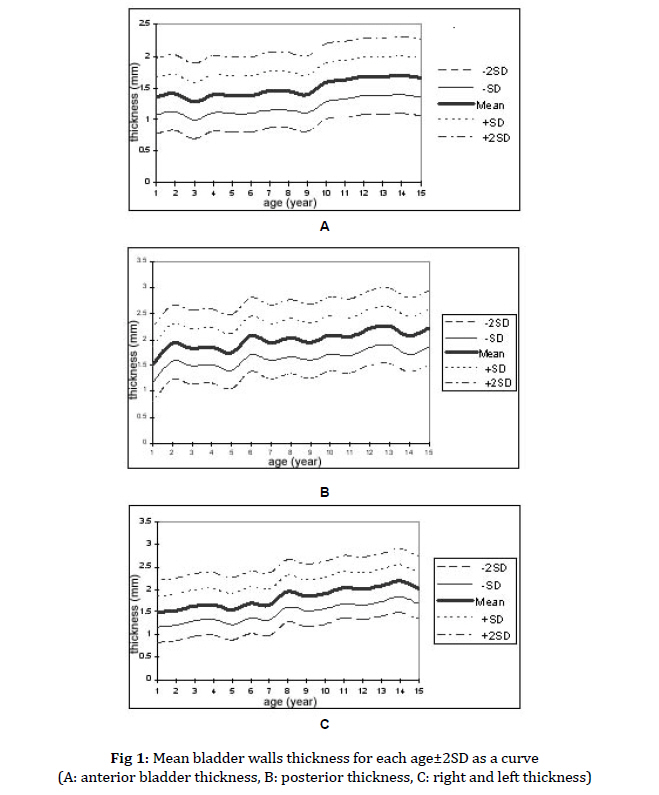
Iranian Journal of Pediatrics, Vol. 19, No. 4, 2009, pp. 341-346 Sonographic Measurement of Bladder Wall Thickness in Healthy Children Hadi Sorkhi1*, MD; Mohammad-Reza Navaeifar1, MD, Haji-Ghorban Nooreddini2, MD; Reza Alizadeh Navaee1, MD; Hamid Shafee3, MD; Abbas Hadipoor1, MD 1. Department of Pediatric, Babol University of Medical Sciences, Babol, IR Iran * Corresponding Author; Address: Department of Pediatric Nephrology, Non communicable Pediatric Diseases Research Center, Amirkola Children Received: Nov 15, 2008; Final Revision: May 16, 2009; Accepted: Jul 06, 2009 Code Number: pe09039 Abstract Objective: The aim of this study was to determine the ultrasonographic (US) bladder wall thickness (BWT) in normal children. Key Words: Children; Bladder wall thickness; Ultrasonography; Bladder Introduction Normal bladder function is needed for micturation and the risk of permanent renal damage (especially in children) is high with abnormal bladder function. Vesicoureteral reflux, bladder outlet obstruction and neuropathic bladder may be associated with morphologic changes of bladder [1-5]. The risk of urinary tract infection and upper urinary tract deteriorations are more with abnormal function of blabber [6-7].So, evaluation of morphology and function of bladder wall is very important in any patient with urinary complaint [8, 9]. Trabeculation of inner surface of bladder can be seen by cyctoscopy or cyctography as a sign of detrusor muscle hypertrophy[10], but these are invasive methods and there is the risk of irradiation by cystography[11]. Transabdominal ultrasonography (US) for evaluation of the lower urinary tract and to assess the bladder wall thickness is a noninvasive and simple method. It has been used during the last few years [12,13, 14]. Mild change in bladder wall can be detected by high frequency ultrasonic transducer (≥7 MHz). But due to lack of consensus about values of bladder wall thickness and different reports (especially in children) on differentiation of normal and abnormal thickness, more studies are needed for an accurate determination of the bladder wall thickness [15,16]. In this study we determined bladder wall thickness by US and assessed the correlation between it and age, sex, weight and height in normal children aged less than 15 years. Subjects and Methods We measured bladder wall points by US in 106 healthy children who had no abnormal history, laboratory or clinical findings of urinary tract. To increase the possibility of obtaining more reliable finding, we matched cases for both age and gender. Inclusion criteria were: age under 15 years, normal urinalysis and culture, no urinary incontinency (children over 3.5 years old) or nocturnal enuresis (children over 5 years old), no history of upper or lower urinary tract disease (urinary tract infections, urgency, frequency), any chronic metabolic or disabling neurological disorders. Before bladder examination, we excluded morphological abnormalities of the urinary tract.Informed consent was obtained from parents of all children. The ethics committee of Babol University of Medical Sciences approved the study. Four points bladder thickness are measured by Siemens (G50) ultrasound scanner with an abdominal transducer of 5 MHz for evaluation of bladder volume, a linear 7.5 MHz (electronic) for under 2-year-olds and a convex 5 MHz for older children. The bladder was visualized in sagittal and transverse view on supine position.After oral hydration, when bladder volume reached more than 50% of its estimated normal capacity and the child needed to void, US examination was performed to determine the bladder fullness by measuring its width (a), the antroposterior diameter (b) and the craniocaudal diameter (c). The bladder volume (V) in milliliters was measured by the formula[16]: V=a×b×c×0.55 assuming that the bladder was spherical. The calculated volume was compared with the normal estimated bladder capacity for age, by the formula [16]: EBC=(age in years ×30) + 30 where EBC is the estimated bladder capacity in milliliters. For each case, bladder fullness ratio was calculated using the formula: Bladder fullness ratio in percent= {(Vobs-Vnorm) / Vnorm} ×100 where Vobs is the observed value and Vnorm is the estimated bladder capacity for age. When bladder volume reached at least 50% of normal bladder volume for age and the child needed to void, four points bladder thickness were measured. Cases, who did not reach this fullness, were asked to drink water until the requested volume was achieved. All determined bladder wall thicknesses were tested with the Komogorov-Smirnov test (for test normality), ANOVA test, Tukey HSD, t-test, paired t-test and Pearson correlation test. The value observed was considered statistically significant when P-value was less than 0.05 (P<0.05). P-value was adjusted by Bonferroni correction test. Findings The study included 106 children (54 boys and 52 girls) and the mean of age was 7.44±4 years (range 8 month to 15 years). The mean thickness of four bladder points was 1.79±0.28 mm, it was 1.82±0.29 mm and 1.75±0.28 mm for boys and girls, respectively (P=0.1). The mean of anterior bladder wall thickness was 1.5±0.3 mm and 2±0.36mm, 1.82±0.34mm, 1.84±0.36mm for posterior, right lateral and left lateral, respectively. There was significant difference between these points (P<0.001) but there was not significant difference between right and left lateral sites (P=0.7). We divided these children according their age to under 5, 5-10 and above 10 years, (table1). and the mean thickness of four bladder points in under 5, 5-10 and 10-15 years were 1.58±0.28 mm, 1.79±0.31 mm, 1.99±0.30 mm respectively (P<0.001). The mean±2.SD thickness of bladder points in children is shown as curves in figure 1 (A-C). The mean height was 119±26 cm (65 to 164 cm), the mean weight was 25.0±12.1 kg (7 to 60 kg) and BMI was 16.0±2.9 (11 to 30). There was significant correlation between height (r=0.596, P<0.001) and weight (r=0.571, P<0.001) with four assessed points of bladder wall thickness but there was no significant correlation between BMI and the points (r=-0.01, P=0.9). Discussion The mean thickness of four bladder points was 1.79±0.28 mm and there was significant difference between all points (P<0.05) except between right and left lateral sites (P>0.05). Many pathological causes such as urinary tract infection, bladder outlet obstruction and neurogenic bladder can influence the bladder wall thickness [17]. Long term bladder outlet resistance by mechanical or functional can lead to increase of thickness, diverticula and disarrangement of uretrovesical junction. The degree of these abnormalities depends on severity of obstruction. There are different methods of investigation on bladder disorders. US is the one that is available, simple, non invasive and without ionization hazard. US, especially using high frequency transducers, makes precise measurement of bladder wall thickness possible[14, 18]. There are few reports on normal bladder thickness in children [14,15,19,20]. Kuzmic et al reported 1.2±0.4 mm, 1.2±0.4 mm, 1.2±0.4 mm and 1.2±0.4 mm for normal detrusor thickness of anterior, posterior, right lateral and left lateral wall, respectively, in 62 children aged 20 months to 18 years [20]. Same as in Kuzmic's findings, there was significant correlation between age and bladder wall thickness in our study, but they did not find a significant difference between bladder wall thickness in four points. Jequier et al assessed total wall thickness and reported 1.55 mm for normal bladder thickness when distended and 3 mm for upper limit of fully filled bladder wall thickness. They reported minimal variation (not significant) between wall thickness and age or gender [21]. Filling more than 50% of expected bladder capacity, Muller and et al reported 1.5 mm for mean detrusor thickness in normal bladder; the anterior detrusor thickness was slightly more in boys than in girls. Although, maximal detrusor and intravesical pressure are higher in boys than in girls, the statistical difference in all children was small and not important [19,22]. In another study Muller et al determined mean anterior and posterior wall detrusor thickness to be 0.9 mm and 1.1 mm [15]. In our study, there was no significant difference between right and left lateral points although other points were statistically different. Uluocak et al determined mean detrusor thickness of anterior, posterior and lateral walls 1.42 mm, 1.57 mm and 1.49 mm, respectively, in healthy school aged children. Same as in our study, they did not find a significant difference between boys and girls [23]. We tried to reach acceptable bladder fullness by oral hydration and found that there is no statistically significant difference in bladder wall thickness when it has reached at least 50% of calculated bladder capacity. This volume seems to be adequate for ultrasonographic evaluation of bladder wall thickness, and it is more comfortable and repeatable especially in children. In this study, there was significant correlation between height and weight with bladder thickness. Although, it seems that more studies are needed for evaluating the correlation between normal bladder thickness with height and weight. There were a few limitations in our study. An accurate estimation of volume was not always possible, because our cases were children and oral intake of water or liquid to reach an acceptable volume was difficult. Another limitation was the difference between lateral and axial resolution of US that may be effective in difference of four points measurements. In fat children there may be reverberation artifact for measurement of anterior bladder wall thickness that must be mentioned. ConclusionWe have estimated normal bladder wall thickness according to age and sex for four wall points and the curve according to age for differentiation of normal and abnormal thickening. We recommend comparing the values of four points measurement with normal±2SD curves according to age. AcknowledgmentWe are grateful to the Research Council and Pediatric Research Center of Babol University of Medical Sciences, which supported this study. References
© Copyright 2009 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe09039t1.jpg] [pe09039f1.jpg] |
| |||||||||

{kind=link}
{kind=link}