 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
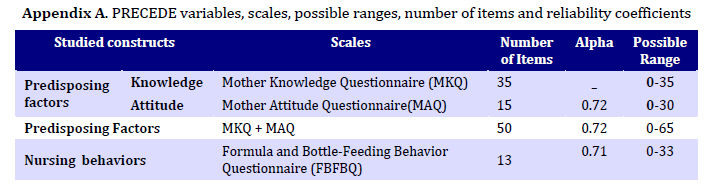
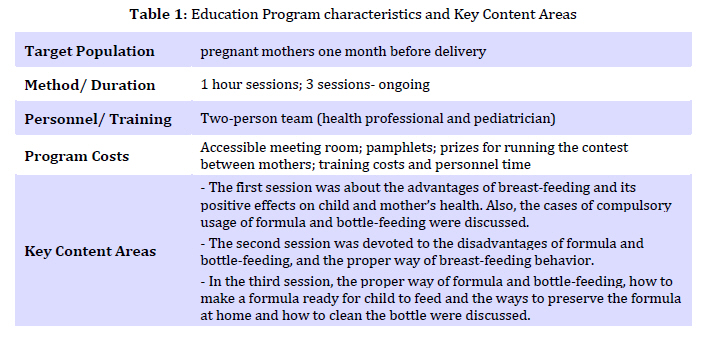
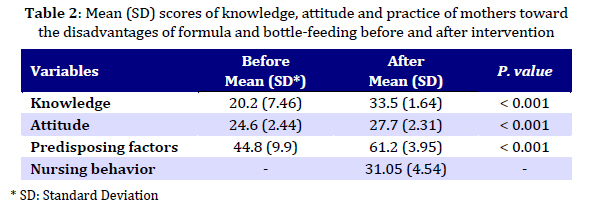
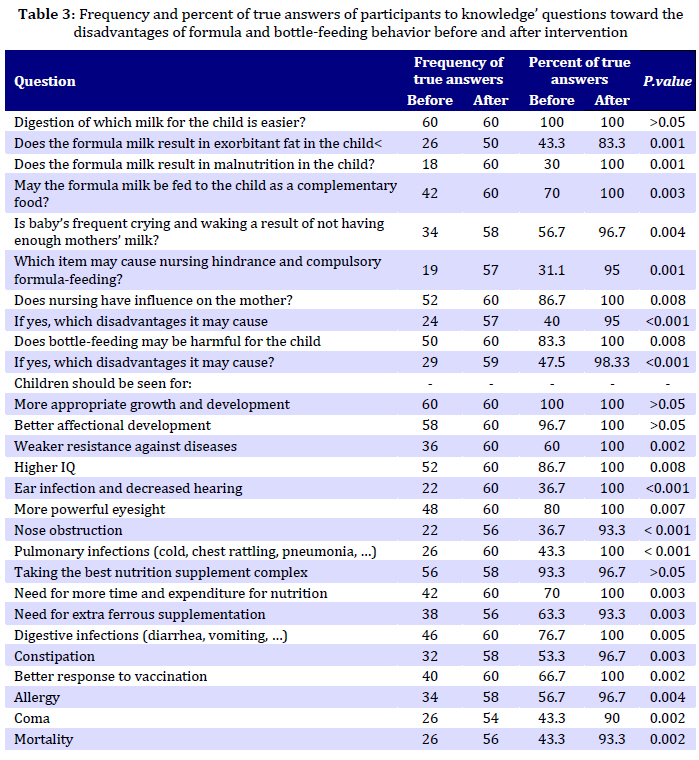
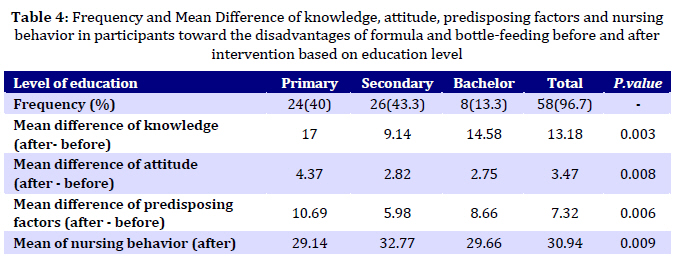
Iranian Journal of Pediatrics, Vol. 19, No. 4, 2009, pp. 359-366 The Effect of Education on Formula and Bottle Feeding Behaviors of Nursing Mothers Based on PRECEDE Model Mohammad-Hossein Baghianimoghadam, PhD; Haidar Nadrian, MSc; Zohreh Rahaei, MScDepartment of Health Services, School of Health, Shahid Sadoughi University of Medical Sciences, Yazd * Corresponding Author; Address: Daneshjo Blvd, School of Health, Shahid Sadoughi University of Medical Sciences, Yazd, IR Iran, E-mail: baghianimoghadam@yahoo.com Received: Feb 05, 2009; Final Revision: May 22, 2009; Accepted: Oct 10, 2009 Code Number: pe09042 Abstract Objective: Although a lot of interventional studies may be found which have investigated the effects of education on nursing mothers regarding advantages of breast-feeding behavior, but very few studies in developing countries have examined whether mothers are conscious of the risks associated with formula and bottle-feeding on children. Knowing that Breast-feeding Index has decreased in Iran and feeding behaviors are not suitable and adequate in nursing mothers, we studied the effect of education based on PRECEDE Model on improving mothers’ breast-feeding behaviors in Yazd, Iran. Key Words: Formula; Bottle feeding; Nursing mothers; PRECEDE model; Education Introduction Breast milk is an elaborate package of chemicals developed over millions of years of primate evolution to promote the newborn's development and build up its defenses against infection. In a 1997 policy statement it declared that "breastfeeding ensures the best possible health as well as the best developmental and psychosocial outcomes for the infant." Moreover, breastfeeding may protect mothers, as well [1]. As part of the US healthy people 2010 objectives, the national health objectives for breastfeeding are to increase the percentage of women who breast feed to at least 75% at birth, 50% at six months, and 25% at 12 months postpartum [2]. But, unfortunately, based on the statistics published by Ministry of Health in Iran, Breast feeding Index has decreased from 47% in 1999 to 23% in 2005. These statistics show that 29.5% of under one year old children are bottle-fed, this is while exclusive breast-feeding till 6 months after birth and not using bottle and formula to feed children is necessary for growth and health[3]. Several studies have shown that the formula-fed children in comparison with breast-fed ones, are more sensitive to childhood widespread diseases like gastroenteritis and a lot of rebellious diseases even in their adulthood (allergy, diabetes, hypertension, lymphoma, etc) and the mortality of formula-fed children is higher as well[2]. Formula-feeding is also a risk factor for Crohn and ulcerative colitis in puberty[4]. The disadvantages of using artificial nutrition like formula and bottle-feeding on the economy of families especially in developing countries are remarkable. In the United States provision of formula milk costs from 500 to more than 1000 dollars for families and in some of the developing countries this cost comprises more than 100% of annually income of the families [5]. Formula-fed children are more likely to be exposed to pathogens, which may contaminate bottles, formula and the food given to the child [6]. Pediatric researchers estimate that 250 to 300 infants die each year from diarrheal infections as a result of bottle-feeding [1]. In a study in Sri Lanka, there was found that non-exclusive breastfeeding rather than exclusive breastfeeding can increase the risk of dying due to diarrhea and pneumonia among 0-5 month old infants by more than two-fold [7]. While feeding the child with bottle, the milk which has no disinfectant factor, may be polluted with microorganisms. The formula is sometimes too diluted before being fed to the child and this may result in more malnutrition and, consequently, retardation in growth of the child. Moreover, children who are not breast-fed are at greater risk for early childhood dental caries [8]. Bottle-feeding results in Baby Bottle Tooth Decay (BBTD) which is manifested as severe dental caries in the primary dentition. There is reported that the prevalence of BBTD ranged between 17 and 85 percent with a mean of 53 percent [9] and its resulted costs is estimated between US$ 1000-2000 per child [10]. Although a lot of interventional studies may be found which have investigated the effects of education on nursing mothers regarding advantages of breast-feeding behavior, but very few studies in developing countries have examined whether mothers are conscious of the risks associated with formula and bottle-feeding on children and whether they understand the implications of performing these behaviors on both child and mother. Changing behavior is related to the topics such as knowledge, training, attitude and motivation. Having problems in these aspects is a serious obstacle for managing behaviors[11]. Therefore, in order to well managing of feeding behaviors in nursing mothers, especially in a developing country like Iran, we should have a comprehensive knowledge about the associations between these aspects and feeding behaviors. An aim of this study was to determine that how knowledge and attitude, as predisposing factors, and training the nursing mothers may affect feeding behaviors in them. The PRECEDE planning model developed by Green and Kreuter[12] provides a systematic process for planning, delivering and evaluating health promotion programs for defined populations. The process takes into account the multiple factors that shape health status and helps planners arrive at a focused subset of those factors for interventional targets. The PRECEDE planning process has been applied to a wide range of health promotion topics, yet we uncovered no application of the model in addressing the effects of education on formula and bottle-feeding behaviors and their predisposing factors in nursing mothers. Predisposing factors (like knowledge and attitude) are a general category of the three general categories of factors affecting individual or collective behavior which form the fourth stage of PRECEDE model (the ecological and educational diagnosis) and are antecedents to behavioral change that provide the rationale or motivation to the behavior. For most health programs, an initial focus on the predisposing factors is the logic order[12]. Educational programs need a suitable framework for education, which PRECEDE model possesses. Knowing that Breast-feeding Index has decreased in Iran and feeding behaviors are not suitable and adequate in nursing mothers, we studied the effect of education based on PRECEDE Model on improving mothers’ breast-feeding behaviors. Subjects and Methods This was a self-controlled quasi-experimental trial. Cluster stage sampling was employed to recruit 60 pregnant mothers one month prior to delivery. The estimation of sample size based on literature review, where P=0.65, d=0.05. The power of the study was 80%. The level of significance was set, a priori, at .05. In the first stage of sampling two healthcare centers were selected randomly, and in the second stage, the mothers at the eighth month of their pregnancy were selected (census) to participate in the study. This entire group received educational intervention. The purpose of the study, which included the mothers’ rights as human subjects for a research study, was explained to them and all signed consent forms. Measures: A panel of experts, consisting of three scholars in the areas of health behavior and education, and a pediatrician, assessed the content validity of the instruments by evaluating the appropriateness and relevance of the items, face validity and response format. The feedback from the panel of experts was used to revise and modify the instruments, which were then pilot tested by a 10 sample of pregnant mothers who were not real samples, to examine their utility (α=0.712). The scales, number of items, reliability coefficients, and possible ranges of the constructs are listed in Appendix A. At the end of questionnaire we asked mothers an additive question regarding their source for getting information about the disadvantages of formula and bottle-feeding as well as the best way for child feeding. The possible answer consists: -Mass media (radio and T.V), relatives, healthcare providers, books and magazines, internet, and physicians. At first, the self-administered questionnaire was completed by all respondents and the data were analyzed by SPSS software; based on the results of this analysis, the problem and weak points of mothers regarding formula and bottle-feeding were distinguished, educational program was designed and implemented as follows: 1) Direct education: Group discussions and techniques of adult learning principles were used to train mothers directly. This experimental group was divided into six groups of 10 mothers. Program characteristics and key content areas of the educational program are shown in table 1. During these sessions, we tried to have a good relationship with mothers and prepare them for an active participation in discussions in order to prepare them for learning, reconsidering their ideas, attitudes and changing their behavior. 2) Indirect education: In this part, a pamphlet regarding the disadvantages of formula and bottle-feeding and the advantages of breast-feeding was prepared to help mothers increase their knowledge about nursing behaviors. A copy of the pamphlet was also given to the family members of the mothers. To increase cooperation of the families, a contest was run with 10 questions and given away prizes to 10 mothers who had the highest score. In this way, families had enough information to persuade mothers to apply safe nursing behaviors. After implementing the educational program through group discussion, lectures and pamphlet after 3 months the questionnaire was again completed by the respondents. The Statistical Package for the Social Sciences (SPSS) was used for the purpose of data entry, manipulation, and analysis. The statistical analyses of data included bivariate correlations, t-test, ANOVA, Man-Whitney, Kruskal-Wallis and Chi-squre. Findings Mean age was 25.9 (SD 5.8) years; 96.6% were housewives, 41.4% had primary school, 44.8% secondary school education and 13.8% university education. There was a significant relationship between using formula-feeding and mother’s level of education (P=0.01) and number of children they had (P=0.01). Moreover, using bottle to feed the children was significantly higher in mothers with more children (P=0.001). There was no significant difference between the child's sex and attitude, knowledge and practice of mothers. Mean and standard deviation scores of knowledge, attitude and practice of mothers in Yazd toward the disadvantages of formula and bottle-feeding before and after education are shown in table 2. After implementing the educational program, mothers' knowledge and attitude were significantly increased (P<0.001). Table 3 shows frequency and percent of true answers of mothers to knowledge questions toward the disadvantages of formula and bottle-feeding behavior before and after education. Before implementing the educational program there was a significant relationship between the respondents' knowledge and attitude with their level of education (P=0.001) in a way that mothers who had secondary school education, showed higher knowledge and attitude than mothers who had primary level of education but this difference was not seen after implementing educational program (Table 4). By asking the informational source of respondents regarding the disadvantages of formula and bottle-feeding before implementing program, 46.7 % of the mothers announced that they used mass media (radio and TV), 40% were guided by relatives, 23.3% were guided by healthcare providers, 16.7% used books and magazines, 3.3% used internet and 3.3% were guided by physicians. After education, the measure of acquiring information from these sources increased, especially acquiring information from healthcare providers increased 100 percent.After implementing the program, 85% of the mothers fed their children exclusively with mother's milk and 15% used both breast-feeding and formula feeding. The children, who were formula-fed, were breast-fed 4-5 times daily as well. Moreover, none of them were formula-fed from the time of birth and formula-feeding was used as a result of improper weight gain in these children. Discussion Results showed that after implementing the educational program, mothers' knowledge and attitude were significantly increased and after delivery only 15% of the mothers used formula-feeding in addition to breast-feeding meanwhile, based on Ministry of Health's statistics in Iran, Breast feeding Index has decreased from 47% in 1999 to 23% in 2005 and bottle-feeding is used for 29.5% of under 1 year old [3]. It is thought that the implemented educational program has had great impact on mother’s knowledge, attitude and breast-feeding behavior. Similar to the findings of the present study, in a study reported from Chili using group discussion and lecture, the amount of breast-feeding in mothers who participated in an educational program during pregnancy, compared with the amount of breast-feeding in those who did not participate in the study, a great increase was seen in exclusively breast-feeding till 6 months from 31.6% to 66.8% and nursing amenorrhea period increased from 22% till 180 days to 56%[13]. In another study there was found that with performing educational intervention, the improper behaviors of mothers regarding the feeding of their children may be modified and prevent the children from being bottle-fed [14]. Regarding the low knowledge level of mothers toward the effect of formula-feeding on malnutrition and increasing the risk of infection in children as well as the low level of knowledge of mothers toward the nursing prohibition in children, it can be said that although mothers have some information about the benefits of breast feeding, they don’t have a proper and clear perception of formula milk disadvantages. This should be considered while designing educational programs for these mothers. The results of this study showed that before implementing the educational program there was a significant relationship between the respondents' knowledge and attitude with their level of education. This finding is clear evidence to positive role of education in increasing knowledge and changing the attitude of individuals. Implementing the educational program, the essential information provided for the mothers and their knowledge and attitude improved significantly. Therefore, there was no significant difference seen between knowledge and attitude of mothers after implementing the program. In our study, before program a few numbers of mothers had used book and magazines, internet to acquire information about disadvantages of formula and bottle-feeding while about half of them have heard some information about this problem from relatives. These findings show the low usage of important informational sources like books, magazines and internet in our society. We can conclude that the mothers in our society are quite easily influenced by information received from their relatives that may be a result of flectional relationship and the existing confidence between them. Therefore, if the proper information in this field is not provided in due time, they will be influenced by either right or wrong knowledge, desires or behaviors of relatives. In a study within which the demographic characteristics and attitudes of 42 mothers who used bottle-feeding was compared with those of 42 mothers who breast-fed their children, breast-feeding among the friends of mothers who breast-fed their children was significantly higher than mothers who bottle-fed their children[15]. Moreover, the results of another study in Glascow showed that the social network members may influence the mother’s feeding choices [16]. After program, acquired information by mothers from different informational sources especially health care providers increased significantly. This shows that the educational program had resulted in increasing the susceptibility of mothers in this field and increasing their motivation toward acquiring more information from available sources. In studies from 9 countries of South America which have widespread programs to propagate breastfeeding, was shown that healthcare system may have an important role in this field [17]. In another study there was found that the mothers with lower level of education used formula-feeding for their children more than the other mothers [15]. This finding proves the role of education in continuing the proper behaviors. The mothers who had more children used formula and bottle-feeding more than the others. It is obvious that by increasing the number of children, the physical and psychological pressure on mother will be elevated and little time remains to satisfy the needs of every child. Keeping in mind that most of mothers decide on their method of feeding prior to delivery, and complications during and following delivery do not alter their plans significantly[15], and not repeating all of the realties about feeding the children, will deprive the parents from making an aware full decision [18], implementing such educational programs for pregnant mothers and their husbands, which beside the advantages of breast feeding for mother and child contains comments on disadvantages of formula and bottle-feeding, is necessary. Conclusion Based on the results of this study, we can propose that in order to design effective educational programs, healthcare professionals should better understand the determinants of feeding behaviors in nursing mothers and develop stage-specific interventions, within which, promoting predisposing factors like knowledge and attitude are priorities of the program. The PRECEDE Model, as a basic model for programming, was found to be helpful in assessing the relationships between predisposing factors and feeding behaviors of nursing mothers as well as addressing the effects of education on formula and bottle-feeding behaviors and their predisposing factors in nursing mothers. We conclude that this model may be used in developing countries, as a framework for planning intervention programs in order to predict and improve the feeding behaviors of nursing mothers. Acknowledgment Financial support for undertaking the survey was provided by the School of Public Health, Shahid Sadooghi University of Medical sciences, Yazd, Iran. We gratefully acknowledge the contributions of the staff of Healthcare Centers, in the collection of data. Our special thanks to Mrs Ranjbar and Dr Taghvaee for their valuable input during the study. References
© Copyright 2009 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe09042t2.jpg] [pe09042t1.jpg] [pe09042t4.jpg] [pe09042t3.jpg] [pe09042a1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}