 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
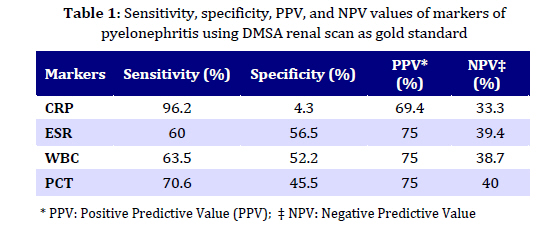
Iranian Journal of Pediatrics, Vol. 19, No. 4, 2009, pp. 381-386 Comparison of Procalcitonin and C-Reactive Protein Tests in Children with Urinary tract infection Parviz Ayazi* 1, MD; Abolfazl Mahyar1, MD; Hassan Jahani Hashemi2, MD; Mohammad-Mahdi Daneshi1, MD; Toktam Karimzadeh1, MD; Fatemeh Salimi1, MD 1. Department of Pediatrics, School of Medicine, Qazvin University of Medical Sciences, Qazvin, IR Iran * Corresponding Author; Address: Qazvin Children Hospital, Qazvin University of Medical Sciences, Qazvin, Iran E-mail: parviz_ayazi@yahoo.com Received: Feb 20, 2009; Final Revision: Jul 23, 2009; Accepted: Aug 16, 2009 Code Number: pe09045 Abstract Objective: Urinary tract infection (UTI) is a common disease in children. The distinction between upper and lower UTI in children is associated with some ambiguities. The objective of this study was to determine the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of procalcitonin (PCT) compared to C-reactive protein (CRP) in predicting renal involvement.| Key Words: Pyelonephritis; UTI; Procalcitonin; Serum marker; Children; C-reactive protein Introduction Young children are at greater risk of acute renal injury following Urinary tract infection (UTI) compared to children of higher age [1,2]. UTI is a common disease in infants and children with a prevalence rate of 6.5 and 3.3% in girls and boys younger than one year of age, respectively [3,4]. Infection could be either limited to the lower urinary tract or extend to the kidneys causing pyelonephritis[4]. While the lower urinary tract infections are usually of no long-term sequelae[4], the infections of upper urinary tract (ie pyelonephritis) could result in renal injury with subsequent renal scarring. This could lead to long-standing medical problems including uremia, arterial hypertension and renal disease at later stages [5]. Precise diagnosis of the location of UTI is of major importance as it affects the type, duration, and the route for administration of antimicrobial therapy and decision making on hospitalization [1,3,6,7]. The potential risk for occurrence of renal parenchymal damage in pyelonephritis makes it a prime necessity to perform more aggressive therapy, investigation and follow-up than does lower UTI[8]. PCT, a propeptide of calcitonin with 116 amino acids and devoid of hormonal activity, was initially described to have the potential of being a marker of bacterial infection[4,9]. Serum concentration of PCT increases in patients with septic shock and is normal in patients with non-infectious inflammatory conditions or viral infections[4]. While low level of PCT is present in serum of a healthy individual (<0.1 mg/l), the titer of this marker will considerably increase (up to 1700-fold) in response to bacterial endotoxins[8]. The "acute-phase response", an intricate response of the organism to tissue injury, infection and inflammatory diseases, is manifested by increased synthesis of hepatic acute phase proteins, including CRP[10]. Measurement of serum CRP level as an important laboratory test for diagnosis and monitoring of different inflammatory processes is well-documented. Considerable rise in concentration of CRP occurs during any clinical disease characterized by tissue injury and/or inflammation [10]. Although elevated level of CRP could be suggestive of infection, nevertheless it fails to provide confirmatory evidence on presence of pyelonephritis in a patient [1,11,12]. The radionuclide evaluation of renal function helps to differentiate between cystitis and pyelonephritis. DMSA renal scan is the method of choice for identification of renal lesions secondary to acute inflammation of parenchyma. Although the imaging techniques could be also used in diagnosing acute upper UTI, they are not cost-effective protocols and expose the patient to radiation[1]. A decisive diagnostic test to distinguish lower UTI from acute pyelonephritis is of great help in management of disease. Hence, the present prospective study was attempted to determine the diagnostic value of serum PCT compared to CRP in predicting renal involvement in infants and children with UTI. Subjects and Methods In this prospective study of 22 months duration, 111 children with median age of 19 months (range 2 to 144 months) were included in the study on admission to the pediatric department of Qazvin Children’s Hospital affiliated to Qazvin University of Medical sciences, Qazvin (Iran), during 2006-2007. All patients were suspected of having UTI (based on clinical findings and active urinalysis, U/A). Children given an antibiotic agent within the previous week were excluded. Inclusion criteria were fever of unknown origin, vomiting, decreased appetite and irritability for infants; abdominal pain and voiding frequency with or without fever for toddlers; and dysuria, frequency, urgency and abdominal or flank pain with or without fever for older children. On admission, all clinical procedures to be used for patients were fully explained and signed written agreement received from parents and kept in patient’s medical record in hospital. Children were given complete physical examination by a single pediatrician followed by collecting 2 ml of venous blood sample prior to initiation of intravenous antibiotic treatment. Serum concentrations of procalcitonin and CRP, complete blood count (CBC), ESR, and urine culture were evaluated. Children diagnosed with UTI were treated with appropriate antibiotic according to the result of antimicrobial susceptibility testing. The EDTA-blood samples were used for measuring PCT, CRP, ESR and CBC. PCT levels were determined by rapid semi-quantitative immunochromatographic method (Brahmas PCT-Q, BRAHMAS Diagnostica, Germany) by a single observer. Briefly, following addition of 200 µl of EDTA plasma to the test strip, PCT present in the sample was bound to mouse anti-catacalcin antibodies conjugated with colloidal gold to form a complex. This complex moved by means of capillarity through an area containing fixed anti-calcitonin antibodies to form a sandwich complex which became visible as a reddish band. The color intensity was indicative of PCT concentration in the sample(4). CRP concentration was also determined by rapid immunometric methods (quantitative test kit for CRP, Parsazmun Co. Tehran, Iran) according to the manufacturer's instruction with values greater than 10 mg/L considered as abnormal. ESR was measured by Westergren method [13]. Different methods including clean-void midstream catch, suprapubic aspiration or sterile urine collection bags were used to collect urine samples, accordingly. All urine samples were immediately transferred to the hospital laboratory and cultured in less than an hour. The bladder tap was performed one hour after feeding. Specimens were analyzed by standard U/A. To obtain standard U/A, specimens were centrifuged at 2000 rpm for 10 minutes and examined microscopically for pyuria (reported as the number of leukocytes per high-power field (HPF)). Pyuria was established by presence of at least 5 leukocytes per HPF. Quantitative urine cultures were performed according to standard technique. If the culture resulted in more than 104 colonies of a single pathogen, or if it was 104 colonies with the child showing urinary symptoms, it was diagnosed as UTI [14]. Statistical analysis: Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for the increased PCT and CRP in serum samples of patients with a positive DMSA scintigraphy as validating standard. Results were reported as the mean±SD. Statistical analysis was performed using Chi-Square test, Mann Whitney test, Fisher's exact test, and t-test with P-value of less than 0.05 considered as significant. Findings This prospective study included a total of 111 children, among those 21 (18.9%) were boys and 90 (81.1%) girls. The age of patients ranged between 2 months and 12 years with a mean age of 34.69±33.6 months. Sixty four patients (57.7%) were <2 years and 47 (42.3%) older than 2 years. The most frequent signs and symptoms were fever (63.1%), dysuria (40.5%), vomiting (27%), bad odor of urine (22.5%), abdominal or flank pain (20.7%), and diarrhea (18.9%). Of 111 patients suspected of having UTI, 46.3% were found to have positive urine culture and 53.7% had negative results. Of 46.3% of children with definite diagnosis of UTI (positive urine culture) 94% had CRP >10mg/L, 87.2% pyuria, 70% increased level of serum procalcitonin, 58% fever, 57.1% ESR >10mm/h, and 56% peripheral WBC count >10000/ml. Fifty two (46.8%) children were revealed to be positive for renal DMSA scan compatible with an acute pyelonephritis (among those 69.2% with fever), 23 (20.7%) children with normal DMSA scan diagnosed as having lower urinary tract infection, and 36 (32.5%) refused to have DMSA renal scan. Comparison of children with pyelonephritis and those with cystitis showed no statistically significant difference for age (32.4±34.0 vs. 37.2±32.0 months, P=0.6), sex (male to female ratio: 11(21.2%)/41(78.8%) vs. 3(13%)/20(87%), P=0.406). WBC count (12111±4206 vs. 11513±6503 P=0.6), and PMN count (64.29±16.2 vs. 64.35±18.0, P=1) between the two groups. The mean concentration obtained for CRP was not significantly higher in children with upper UTI compared to children with cystitis (27 vs. 23 mg/dl, P=0.7). In addition, in 2 (3.8%) children with cortical defect on renal DMSA scan, the CRP values were normal. Also, higher concentrations of CRP were observed in 22 (30.6%) children in whom no renal cortical involvement was found. Comparatively, blood PCT was negative in 15 (60%) children with pyelonephritis and positive in 12 (54.5%) with cystitis. As the clinical benefit of a diagnostic test is mainly measured by the accuracy with which a test identifies its target disorder and is best approached through calculation of the likelihood ratio (LR)[4], it could be set forth that the positive predictive value of procalcitonin can predict the presence of pyelonephritis in 75% of cases (LR=1.29), while by a CRP concentration >10mg/l the prediction of pyelonephritis is about 69.4% (LR=1.005). Considering the DMSA renal scan as the gold standard for pyelonephritis, the sensitivity, specificity, PPV, and NPV obtained for CRP, ESR, WBC count, and PCT were calculated (Table 1). Discussion Pyelonephritis must be distinguished from lower UTI as it could lead to chronic renal damage and, in case of extensive renal scarring, arterial hypertension and renal insufficiency[8]. In present work, we used an extremely sensitive technique to assess renal parenchymal involvement[3,4]. Kidney DMSA scintigraphy is capable of distinguishing pyelonephritis from lower UTI and it is now considered to be the reference method for diagnosis of renal involvement[8]. DMSA renal scan was performed during the acute phase of infection and based on our data, 46.8% of children were found to suffer parenchymal defect among those 69.2% with fever. These results are in agreement with findings of two studies in which 67 and 61.9% of infants and children with symptomatic febrile UTI were reported to have renal involvement[15,16]. However, scintigraphy is an expensive diagnostic procedure, unavailable in many medical centers worldwide with the risk of exposing the patients to radiation. In addition, it would be most valuable to progress rapidly in differentiation between lower UTI and acute pyelonephritis, eg through the use of inflammatory markers. In current study, attempts were made to investigate the possible correlation of a blood marker with DMSA renal scan. A new rapid semi-quantitative test for PCT has become available and could be a useful tool for management of UTI. In addition to procalcitonin, we also tested CRP quantitatively and compared the results with those of PCT to differentiate between pyelonephritis and lower UTI. Renal lesions were observed in 46.8% of children with CRP sensitivity and specificity of 96.2 and 4.3%, respectively. In a study by Benador the sensitivity and specificity calculated for CRP were 100% and 26.1%, respectively[8]. In one recent study by Pecile, a sensitivity of 94.4% and specificity of 31.9% for CRP was reported[17], which is relatively compatible with the results of our study. The high sensitivity of CRP in different studies shows that most children with normal CRP values could be safely considered as unaffected by acute pyelonephritis and would not require either DMSA scintigraphy or early parenteral antibiotic therapy. However, a number of children with elevated concentrations of CRP showed no renal lesion, reflected in low (4.3%) specificity of the test, which limits the clinical usefulness of CRP, leading to unnecessary hospital admissions and costs. The sensitivity and specificity of PCT in our study were 70.6% and 45.5% respectively. These results are inconsistent with findings of a study by Pecile who reported a sensitivity and specificity of 83.3% and 93.6% for PCT, respectively. In another study by Geravix a relatively similar figure for sensitivity (74%) but a different specificity (85%)[4,17] compared to our data were found. Among 46.8% of children with renal parenchymal involvement, 70.6% were demonstrated having elevated PCT level and 29.4% having it within the normal range. This could be the result of the time lag between PCT determination and DMSA renal examination in children who came to hospital shortly after the onset of symptoms. These results are in accordance with the study carried out by Pecile (in which 73.5% of patients with elevated PCT level showed renal parenchymal involvement and 9 with normal PCT involvement of renal parenchyma). During this time lag (onset of symptoms and medical seek), the inflammation induced by the infection can progress and lead to proximal tubular dysfunction, resulting in abnormal DMSA renal scan[4]. The PPV and NPV values for PCT, found in present study, were 75% and 40%, respectively, which are somehow different from those shown by Galetto-Lacour et al, where the values obtained for PPV and NPV were 60% and 96%, respectively. In the same way, the PPV and NPV figures calculated for CRP were 69.4% and 33.3%, respectively, while those by the same researchers showed relatively similar PPV (61%) but different NPV (90%) values[18]. Comparing the low specificity obtained in present research with higher specificity found by others, it seems that several factors including different population size and age, diverse races and genetic background, and also application of various commercial diagnostic kits could affect the results of any research of this kind. This could be the basis of further researches in which the question of whether the race variation might produce different results to be investigated while using the same commercial laboratory kits and larger scale experiments. Thus, this could be regarded as the limitation of the present study. Conclusion Our data indicated that PCT is a better biological marker in predicting acute pyelonephritis among infants and children, compared with low specificity of CRP. Thus, determination of blood procalcitonin level could be more useful, in comparison to CRP for management of children with UTI. Acknowledgment This project was financially supported by the Research Department of Qazvin University of Medical Sciences (Project Code: 239). We would like to thank the research council and also the vice chancellor for research department. Similarly, we thank Dr Ali Pahlevan for his meticulous revision of the original manuscript. Our regards also go to the staff of Qazvin Children's Hospital and Miss Jila Pourrezaei for their assistance. References
© Copyright 2009 - TUMS PUBLICATIONS The following images related to this document are available:Photo images[pe09045t1.jpg] |
| |||||||||

{kind=link}